| Journal of Current Surgery, ISSN 1927-1298 print, 1927-1301 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Curr Surg and Elmer Press Inc |
| Journal website https://jcs.elmerpub.com |
Case Report
Volume 16, Number 1, June 2026, pages 20-26

Re-Inventing the Bicycle: A Modification of the Sauve-Kapandji Procedure
Kaspars Silinsa, b ![]() , Dominique Nellie Merkya, Esther Voegelina
, Dominique Nellie Merkya, Esther Voegelina
aDepartment of Plastic and Hand Surgery, Inselspital, University Hospital of Bern, 3010 Bern, Switzerland
bCorresponding Author: Kaspars Silins, Inselspital, University Hospital of Bern, 3010 Bern, Switzerland
Manuscript submitted September 8, 2025, accepted February 3, 2026, published online May 22, 2026
Short title: Modification of the SK Procedure
doi: https://doi.org/10.14740/jcs1013
| Abstract | ▴Top |
The Sauve-Kapandji (SK) procedure is a well-established treatment for distal radioulnar joint (DRUJ) osteoarthritis and instability, but long-term instability of the proximal ulnar stump remains a common cause of pain and functional limitation. Soft tissue stabilization techniques, particularly using an extensor carpi ulnaris (ECU) tendon slip, have shown reliable long-term outcomes. Another frequent complication is heterotopic ossification or synostosis at the osteotomized non-union site, which restricts forearm rotation. Pyrolytic carbon implants, known for their biocompatibility, durability, and favorable mechanical properties, have demonstrated success in small joint arthroplasty. We describe a novel modification of the SK procedure using a PyroDisk™ implant interposed at the distal ulnar osteotomy to maintain the non-union gap, combined with ECU tendon stabilization to improve proximal ulnar stump stability. We report three clinical cases treated with this modified SK technique, demonstrating significant improvements in pain relief, range of motion (ROM), grip strength, and stability at an average follow-up of 14 months. Radiographic evaluation showed maintenance of the osteotomy gap without recurrent ossification or implant-related complications. These preliminary findings suggest that this modification could provide a promising alternative to traditional SK techniques, potentially overcoming major limitations related to instability and synostosis. Written informed consent was obtained from all patients prior to surgery.
Keywords: Rheumatoid arthritis; Madelung deformity; DRUJ; Sauve-Kapandji
| Introduction | ▴Top |
The Sauve-Kapandji (SK) procedure is a well-established surgical technique for managing distal radioulnar joint (DRUJ) osteoarthritis and instability, originally described by Sauve and Kapandji in 1936 [1]. Despite its widespread adoption and numerous technical modifications, achieving long-term stability of the proximal ulnar stump remains challenging, often leading to persistent pain, weakness, and functional limitations [2]. To address these issues, various soft tissue stabilization methods have been explored, with the extensor carpi ulnaris (ECU) tendon slip showing promising long-term clinical outcomes as a reliable stabilizer [3]. However, a common complication associated with the SK procedure is recurrent heterotopic ossification or synostosis at the non-union site, which restricts forearm rotation and may cause symptom recurrence [4].
Pyrolytic carbon (PyroCarbon) implants have gained attention in small joint arthroplasty due to their excellent biocompatibility, wear resistance, and favorable mechanical properties, demonstrating promising durability and patient tolerance [5]. Inspired by these advantages, we developed a novel modification of the SK procedure inserting a PyroDisk™ implant interposed at the distal ulnar osteotomy to maintain the non-union gap, combined with dynamic stabilization using a slip of the ECU tendon. We present three clinical cases that were treated using this modified SK technique.
| Case Report | ▴Top |
Between May 2022 and December 2023, three selective female patients, aged 27 to 52 years, with symptomatic DRUJ osteoarthritis or instability, underwent the modified SK procedure incorporating a PyroDisk™ implant and ECU tendon slip stabilization. Two of these patients had underlying autoimmune inflammatory arthritis (rheumatoid arthritis and juvenile idiopathic arthritis), adding complexity due to chronic synovitis and compromised soft tissue quality.
A 27-year-old woman with a 7-year history of seropositive rheumatoid arthritis presented with progressive right wrist pain localized to the ulnar side of her right dominant wrist and marked loss of pronation and supination. Despite disease-modifying therapy with baricitinib (Olumiant®), she developed DRUJ instability and dorsal ulnar subluxation. Previously, she underwent radioscapholunate arthrodesis and triangular fibrocartilage complex (TFCC) reconstruction by the Brian-Adams technique [6], but persistent pain and reduced grip strength remained. A clinical examination revealed tenderness over the DRUJ, as well as painful pronation and supination, diminished radial and ulnar adduction (5° in each direction) and grip weakness. Corticosteroid infiltration (Depo-Medrol®) of the ulnocarpal joint provided transient relief but failed to improve function. Imaging showed advanced DRUJ osteoarthritis with subluxation. Due to persistent symptoms refractory to conservative management, she was scheduled for the modified SK procedure with PyroDisk™ interposition.
A 35-year-old woman with a diagnosis of juvenile idiopathic arthritis on etanercept (Enbrel®) presented with disabling ulnocarpal pain of her left dominant wrist and limited forearm rotation. Her childhood history included proximal radial head subluxation corrected by ulnar lengthening with an Ilizarov fixator at age 11, followed by partial radial head resection via Outerbridge-Kashiwagi procedure [7] to address persistent proximal radioulnar joint (PRUJ) pain. These interventions led to an ulna-plus variant resulting in distal ulnocarpal impingement and DRUJ osteoarthritis. Despite splinting and non-steroidal anti-inflammatory drugs (NSAIDs), she reported significant pain and functional restriction. Clinical examination confirmed ulnocarpal tenderness and restricted rotation (pronation 50° and supination 35°, respectively). Radiographs demonstrated ulna-positive variance with degenerative changes at the DRUJ. The decision was made to proceed with the modified SK procedure incorporating PyroDisk™ and ECU stabilization.
A 52-year-old woman with a history of Madelung deformity of her right dominant wrist underwent a SK procedure 20 years earlier. Over time, she developed painful ossification at the distal ulnar pseudarthrosis site, severely limiting pronation (10°) and supination (20°). The resulting pain and stiffness significantly impaired her activities of daily living. Radiographs revealed exuberant heterotopic ossification bridging the pseudarthrosis. Given the chronicity and severity, she was offered revision surgery using the modified technique to restore motion and alleviate pain.
None of the patients were smokers. All procedures were performed under regional anesthesia with the patient supine and arm on an arm table. A longitudinal incision over the fifth extensor compartment provided access to the DRUJ. Careful soft tissue dissection exposed the distal ulna and sigmoid notch. The DRUJ was arthrodesed by fusing the sigmoid notch to the distal radius to eliminate painful joint movement, as originally described in the SK procedure [1]. A distal ulnar osteotomy was performed to create a pseudarthrosis about 8–10 mm wide to accompany the PyroDisk™. A distally based slip of the ECU tendon (approximately 8 cm in length) was mobilized to act as a dynamic stabilizer of the proximal ulnar stump. Drill holes were created with a 2.0 mm drill in the proximal and distal ulnar stumps adjacent to the osteotomy site. The appropriately sized PyroDisk™ implant was inserted into the osteotomy gap (5.5 mm height, 14 or 16 mm diameter), maintaining the non-union space and preventing bone bridging. The ECU tendon slip was threaded through the drill holes and passed through the central aperture of the PyroDisk™. Through pulling the tendon towards itself, the tension was adjusted and tested intraoperatively (Fig. 1). In two patients, additional FiberTape® augmentation by threading it through the tendon was used to enhance mechanical stability, providing supplementary strength to the ECU tendon construct due to the lack of stability provided by the tendon itself. Intraoperative fluoroscopy and clinical assessment guided the tensioning to optimize stability. The ECU slip was sutured onto itself to maintain tension. Wound closure was performed in layers.
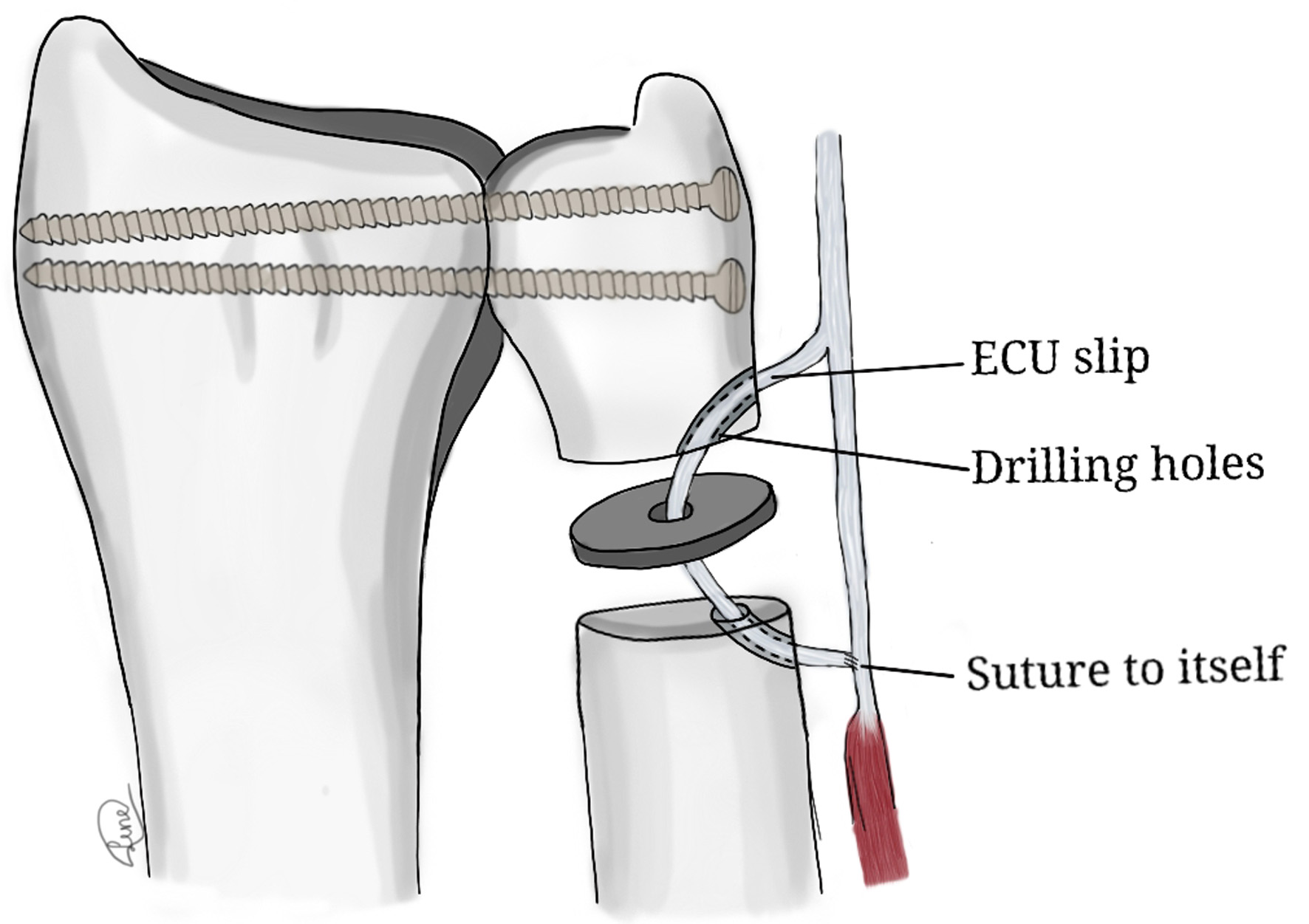 Click for large image | Figure 1. Schematic drawing of the procedure. |
Postoperatively, patients were immobilized in a sugar-tong or Bower’s splint for 8 weeks, allowing wrist flexion-extension in a neutral position from day 1 but prohibiting forearm pro-supination and weight bearing. Passive and active forearm rotation exercises commenced after 4 weeks, gradually increasing range and frequency. Weight bearing was restricted until 8 weeks, followed by progressive loading and removal of the splint at this point. All patients underwent occupational therapy of our institution once a week without missing a session to follow up on the progress of the rehabilitation and providing and supervising the necessary exercises.
At an average follow-up period of 14 months (range 12–19 months), all three patients reported pain relief, improved grip strength, and increased range of motion (ROM) [8] compared with their preoperative status (Table 1). No incidences of infection, implant loosening or recurrent ossification were observed on radiographs. The PyroDisk™ implant remained stable within the osteotomy gap in all cases. Notable total ROM improvements were observed in pronation and supination, with gains ranging from 10° (patient 1) to 85° (patient 2). Grip strength measured with Jamar dynamometer [9] more than doubled in the first patient (from 14 to 30 kg), and improved substantially in the other patients as well. Postoperative radiographs (Figs. 2–5) show that the gap in the distal ulna osteotomy was maintained measuring the distance between both ulnar stumps in both views, without evidence of ossification of the non-union or implant migration at the latest follow-up. The radiological findings were assessed by the surgeon and independent radiologist on duty on the respective day of follow-up. This favorably contrasts with the known propensity for heterotopic ossification after traditional SK procedures [4].
 Click to view | Table 1. Preoperative and Postoperative Clinical Outcome |
 Click for large image | Figure 2. Pre- and postoperative X-rays of the first patient. |
 Click for large image | Figure 3. Pre- and postoperative X-rays of the second patient. |
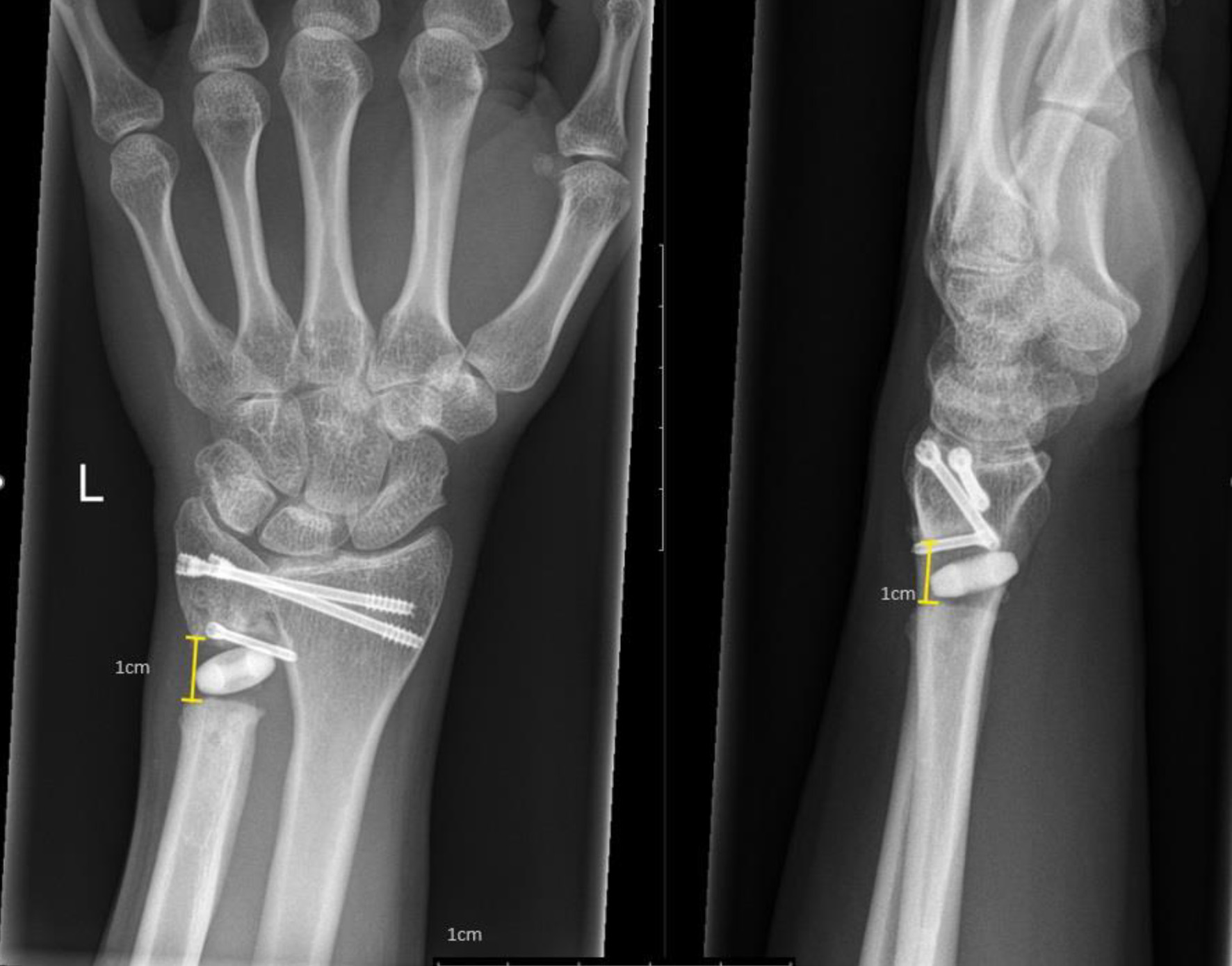 Click for large image | Figure 4. Showing postoperative X-rays with 1 cm gap. |
 Click for large image | Figure 5. Pre- and postoperative X-rays of the third patient. |
A painful DRUJ can lead to a significant restriction in daily activity. Although various options for surgical treatment exist, literature has not shown a clear advantage of a single procedure. The SK procedure offers several theoretical advantages, including maintaining ulnar support of the carpus, the ability to shorten the ulna if necessary, preserving normal force transmission through the wrist and requiring only a relatively short period of immobilization [10].
Pyrocarbon has been successfully used in treating osteoarthritis of the rheumatoid wrist. Lestienne et al published a study with a 5-year follow-up after implanting the Amandys® implant (Wright-Medical, Tornier, Montbonnot Saint Martin, France) for radiocarpal joint arthroplasty. They demonstrated that the pyrocarbon material was well tolerated both clinically and radiologically, with no signs of implant loosening or adverse reactions such as osteolysis. Impressively, their study reported a 100% survival rate of the implant at a mean follow-up of 64 months, highlighting its durability and biocompatibility in a complex inflammatory setting [11].
Lamont et al published a comprehensive review article evaluating outcomes of the SK and Darrach procedures. They found that over 70% of patients achieved satisfactory results following surgery; however, the most common complication encountered was symptomatic ulnar stump instability with both techniques [12]. This persistent issue underlines the need for improved methods of stabilizing the proximal ulnar stump to enhance long-term outcomes. Our preliminary results indicate that the combined use of the PyroDisk™ implant with an ECU tendon slip effectively stabilizes the osteotomy site and preserves the pseudarthrosis, providing a satisfactory clinical outcome. Stability was achieved in all three cases presented.
While the PyroDisk™ itself does not confer mechanical stability, augmentation with the ECU tendon slip, and when necessary with FiberTape®, enhances rigidity. FiberTape® is a braided polyblend suture tape widely used to augment tendon repairs and ligament reconstructions due to its high tensile strength and ability to distribute loads [13]. An in vivo animal study by Soreide et al confirmed that suture tape augmentation improved biomechanical stability in ligament reconstruction, suggesting similar benefits in tendon-based stabilization [13]. Tendon augmentation techniques with suture tape are increasingly common in orthopedic practice, as evidenced by recent reports on quadriceps tendon repair and anterior cruciate ligament reconstruction [14, 15]. In our series, FiberTape® augmentation was added in two out of three patients, excluding the youngest, to enhance stability without compromising soft tissue integrity. The functional results in grip strength and ROM align well with other published data on the SK procedure, indicating that our modification may offer a reproducible and durable solution to the common instability problem.
Giberson et al reported significantly improved patient-reported outcomes (PROs) 1 year after surgery [16]. Our median 14-month follow-up demonstrates the same improvement 1 year after surgery. This observation period is rather short to conclude about accurate patient satisfaction.
There are alternative surgical techniques to assess DRUJ arthritis. The Darrach procedure [17] was not considered due to the age of patients as it is reserved for older patients with lower functional demands [18]. A distal ulnar hemi-resection arthroplasty (Bowers-Procedure) [19] could have been an option, but only in stable DRUJ, which was not the case in these three patients. Furthermore, ulnar stylocarpal impingement associated with pain would have still been a possible issue [18]. A total DRUJ arthroplasty can also be considered, especially in our youngest patient; however, in combination with an unstable DRUJ, only a Scheker prosthesis [20] would have been an option. After failure of our modified SK procedure [21], a conventional ulna head prosthesis is still an option [22].
There are several limitations that warrant discussion. Firstly, the small sample size of three cases limits the generalizability of our findings. Further, larger prospective studies with longer follow-up periods are required to ascertain the longevity of this technique and to monitor for potential complications such as implant wear or loosening over time.
Secondly, the mean follow-up period of 14 months is relatively short compared to previous long-term reports on the SK procedure. The long-term risks of heterotopic ossification, implant failure or ECU tendon attenuation remain controversial, especially in patients with an underlying rheumatological condition. One of our three patients is still under observation. The other two patients refused further follow-up due to the absence of symptoms.
Thirdly, the addition of FiberTape® reinforcement was not the same for all patients, which creates differences in how much the material was used. Man et al reviewed the efficacy of anterior cruciate ligament reconstruction using autograft with or without augmentation and found no advantage in augmenting the graft with regard to PROs, knee laxity or graft failure rate [23].
Lastly, this modification requires surgical expertise in both tendon handling and implant placement, which may limit its adoption without specific training.
Conclusions
This report presents a novel modification of the SK procedure incorporating a PyroDisk™ implant as an interpositional spacer and dynamic stabilization of the proximal ulnar stump using an ECU tendon slip. Our preliminary clinical experience in three patients demonstrates promising outcomes, including significant pain relief, improved ROM, enhanced grip strength, and prevention of recurrent ossification or instability at short-term follow-up. By “re-inventing the bicycle,” this upgraded technique addresses two of the most challenging complications of the traditional SK procedure: proximal ulnar stump instability and heterotopic ossification. While these early results are encouraging, longer-term studies with larger cohorts are required to validate the durability and safety of this approach. Only time will tell if this improved construct will withstand the mechanical demands placed upon the distal forearm, but the combination of a stable, biocompatible implant with dynamic tendon stabilization represents a promising evolution in the surgical management of DRUJ dysfunction.
Acknowledgments
None to declare.
Financial Disclosure
None to declare.
Conflict of Interest
None to declare.
Informed Consent
An informed consent was acquired from all the patients included in this case report.
Author Contributions
Esther Vögelin (EV) conceived and presented the idea. Dominique Merky (DM) and EV conducted the surgeries. All the authors were involved in the follow-up. KS gathered the data and wrote the manuscript, receiving input from all the authors. KS conducted the literature research in consultation with DM and EV. All authors approved the final content of the submission.
Data Availability
The authors declare that data supporting the findings of this study are available within the article.
Abbreviations
DRUJ: distal radioulnar joint; ECU: extensor carpi ulnaris; PROs: patient-reported outcomes; PRUJ: proximal radioulnar joint; ROM: range of motion; SK: Sauve-Kapandji
| References | ▴Top |
- Sauve L, Kapandji M. Nouvelle technique de traitement chirurgical des luxation recidivantes isolées de l’extremite inferieure de cubitus. J Chir (Paris). 1936;47:589-594.
- Reissner L, Schweizer A, Unterfrauner I, Estermann L, Nagy L. Long-term results of Sauve-Kapandji procedure. J Hand Surg Eur Vol. 2021;46(6):626-631.
doi pubmed - Minami A, Iwasaki N, Ishikawa J, Suenaga N, Kato H. Stabilization of the proximal ulnar stump in the Sauve-Kapandji procedure by using the extensor carpi ulnaris tendon: long-term follow-up studies. J Hand Surg Am. 2006;31(3):440-444.
doi pubmed - Lamey DM, Fernandez DL. Results of the modified Sauve-Kapandji procedure in the treatment of chronic posttraumatic derangement of the distal radioulnar joint. J Bone Joint Surg Am. 1998;80(12):1758-1769.
doi pubmed - Barrera-Ochoa S, Vidal-Tarrason N, Correa-Vazquez E, Reverte-Vinaixa MM, Font-Segura J, Mir-Bullo X. Pyrocarbon interposition (PyroDisk) implant for trapeziometacarpal osteoarthritis: minimum 5-year follow-up. J Hand Surg Am. 2014;39(11):2150-2160.
doi pubmed - Adams BD, Berger RA. An anatomic reconstruction of the distal radioulnar ligaments for posttraumatic distal radioulnar joint instability. J Hand Surg Am. 2002;27(2):243-251.
doi pubmed - Kashiwagi D. Intraarticular changes of the osteoarthritic elbow, especially about the fossa olecrani. J Jpn Orthop Assoc. 1978;52:1367-1382.
- Flowers KR, Stephens-Chisar J, LaStayo P, Galante BL. Intrarater reliability of a new method and instrumentation for measuring passive supination and pronation: a preliminary study. J Hand Ther. 2001;14(1):30-35.
doi pubmed - Bohannon R, Peolsson A, Massy-Westropp N, Desrosiers J, Bear-Lehman J. Reference values for adult grip strength measured with a Jamar dynamometer: a descriptive meta-analysis. Physiotherapy. 2006;92(1):11-15.
- Munaretto N, Aibinder W, Moran S, Rizzo M. Sauve-Kapandji remains a viable option for distal radioulnar joint dysfunction. Hand (N Y). 2022;17(5):963-968.
doi pubmed - Lestienne V, Chaves C, Tanwin Y, Loubersac T, Gaisne E, Kerjean Y, Bellemere P. Results of interposition arthroplasty with the Amandys® pyrocarbon implant in rheumatoid wrist at a mean 5 years’ follow-up. Hand Surgery and Rehabilitation. 2021;40(5):579-558.
- Lamont S, Debkowska M, Johnsen P, Froehle A, Cotterell IH, Isaacs J. Outcomes of Darrach and Sauve-Kapandji Procedures: A Systematic Review. Hand (N Y). 2024;19(1):68-73.
doi pubmed - Soreide E, Denbeigh JM, Lewallen EA, Thaler R, Xu W, Berglund L, Yao JJ, et al. In vivo assessment of high-molecular-weight polyethylene core suture tape for intra-articular ligament reconstruction: an animal study. Bone Joint J. 2019;101-B(10):1238-1247.
doi pubmed - Thorne TJ, Dong W, Higgins TF, Rothberg DL, Haller JM, Marchand LS. Primary repair of complete quadriceps tendon rupture with extensor mechanism deficit. JBJS Essent Surg Tech. 2024;14(3):e23.00045.
doi pubmed - Weninger P, Steffel C, Rabel S, Karimi R, Feichtinger X. Anterior cruciate ligament reconstruction using a Fascia Lata Graft with FiberTape augmentation. Arthrosc Tech. 2023;12(1):e127-e133.
doi pubmed - Giberson-Chen CC, Leland HA, Benavent KA, Harper CM, Earp BE, Rozental TD. Functional outcomes after Sauve-Kapandji arthrodesis. J Hand Surg Am. 2020;45(5):408-416.
doi pubmed - Darrach W. Partial excision of lower shaft of ulna for deformity following Colles's fracture. 1913. Clin Orthop Relat Res. 1992;275:3-4.
pubmed - Katt BM, Tawfik A, Zingas N, Sirch F, Beredjiklian PK, Fletcher D. Distal radioulnar joint osteoarthritis: an update on treatment options. J Hand Microsurg. 2023;15(1):5-12.
doi pubmed - Bowers WH. Distal radioulnar joint arthroplasty: the hemiresection-interposition technique. J Hand Surg Am. 1985;10(2):169-178.
doi pubmed - Scheker LR, Babb BA, Killion PE. Distal ulnar prosthetic replacement. Orthop Clin North Am. 2001;32(2):365-376.
doi pubmed - Fok MWM, Fernandez DL, van Schoonhoven J. Midterm outcomes of the use of a spherical ulnar head prosthesis for failed Sauve-Kapandji procedures. J Hand Surg Am. 2019;44(1):66.e1-e9.
doi pubmed - Herbert TJ, van Schoonhoven J. Ulnar head replacement. Tech Hand Up Extrem Surg. 2007;11(1):98-108.
doi pubmed - Man Q, Gao Y, Wang H, Ma Y, Meng Q. There is no difference in the efficacy of anterior cruciate ligament reconstruction using autograft combined with or without ligament augmentation: a systematic review and meta-analysis. Knee Surg Sports Traumatol Arthrosc. 2023;31(12):5524-5534.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (CC BY 4.0), which permits unrestricted use, distribution, and reproduction in any medium, including commercial use, provided the original work is properly cited.
Journal of Current Surgery is published by Elmer Press Inc.