| Journal of Current Surgery, ISSN 1927-1298 print, 1927-1301 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Curr Surg and Elmer Press Inc |
| Journal website https://jcs.elmerpub.com |
Original Article
Volume 16, Number 1, June 2026, pages 1-8

Management and Outcome of Late Post-Pancreatectomy Hemorrhage After Pancreaticoduodenectomy: Experience From a High-Volume UK Tertiary Center
Maria Aleksandra Dobrzyckaa, b ![]() , Nikolaos Chatzizachariasa, Himanshi Bishta, Syed Shadab Razaa, Bobby V. Dasaria, David C. Bartletta, Ravi Marudanayagama, Keith J. Robertsa, Robert P. Sutcliffea, Michail Papamichaila
, Nikolaos Chatzizachariasa, Himanshi Bishta, Syed Shadab Razaa, Bobby V. Dasaria, David C. Bartletta, Ravi Marudanayagama, Keith J. Robertsa, Robert P. Sutcliffea, Michail Papamichaila
aDepartment of Hepatobiliary and Pancreatic Surgery, Queen Elizabeth Hospital Birmingham, University Hospitals Birmingham NHS Foundation Trust, Birmingham B15 2GW, UK
bCorresponding Author: Maria Aleksandra Dobrzycka, Department of Hepatobiliary and Pancreatic Surgery, Queen Elizabeth Hospital Birmingham, University Hospitals Birmingham NHS Foundation Trust, Birmingham B15 2GW, UK
Manuscript submitted December 4, 2025, accepted March 23, 2026, published online May 19, 2026
Short title: Late Hemorrhage After Pancreaticoduodenectomy
doi: https://doi.org/10.14740/jcs1020
| Abstract | ▴Top |
Background: Delayed bleeding after pancreaticoduodenectomy (PD) is a serious complication with significant morbidity and mortality. The aims of the study were to evaluate the incidence, management, and outcomes of late (> 24 h) post-pancreaticoduodenectomy hemorrhage (PPH) after PD in a high-volume tertiary referral center.
Methods: A retrospective analysis of a prospectively maintained database of 1,184 patients who underwent PD between 2011 and 2023 was performed. Patients who developed late PPH were identified. Diagnostic investigations included computed tomography (CT) angiography, invasive angiography, and endoscopy. Interventions included endovascular treatment (embolization and/or stent graft placement) and laparotomy.
Results: Twenty-three patients (1.94%) developed late PPH, at a median onset of 15.6 days after surgery. Of late PPH cases, 62.5% were associated with pancreatic fistula. Eighteen patients (78.3%) underwent endovascular therapy, whilst five patients (21.7%) required surgery. The gastroduodenal artery (GDA) was the most common source of bleeding (43.5%). In-hospital mortality was 17.4%.
Conclusions: Late PPH after PD is a rare but serious complication with a high mortality rate. Early detection with CT angiography and endovascular treatment is effective in managing most cases, reducing morbidity and mortality. Surgery remains a secondary option for refractory bleeding.
Keywords: Pancreaticoduodenectomy; Pseudoaneurysm; Bleeding; Arterial embolization
| Introduction | ▴Top |
Hemorrhage is one of the most serious complications following pancreaticoduodenectomy (PD). The incidence is relatively low (1.5–15%) but the associated mortality remains high (up to 38%) [1]. Recurrent bleeding after initial management can be significant as well (up to 30%) [1]. Bleeding within the first 24 h after the operation is termed early and is usually due to insufficient hemostasis in the surgical field. As per the International Study Group of Pancreatic Surgery (ISGPS) guidelines, any bleeding after the first postoperative day is classified as late and usually occurs within 1–4 weeks [2]. Bleeding can be in the peritoneal cavity or intraluminally within the gastrointestinal (GI) tract and the main contributing factor is pancreatic anastomotic leak. Other causes include vascular wall trauma or thermal injury during dissection, bile leak, mechanical irritation from surgical drains, staple line bleeding or early mucosal ulcers mainly in the stomach often in the region of gastrojejunostomy [3]. The typical scenario is intraperitoneal bleeding due to a pseudoaneurysm formation following pancreatic anastomotic leakage most commonly involving the gastroduodenal artery [2]. Late post-pancreaticoduodenectomy hemorrhage (PPH) commonly presents with a sentinel bleed, defined as evidence of minimal blood loss in the surgical drains or GI tract followed by an asymptomatic interval until the development of acute hemorrhagic shock, and is an important clinical indicator of pseudoaneurysm formation [4].
Currently, angiogram and endovascular treatment with embolization or stenting is considered the first option for definitive management for late PPH. Surgery may also be required, and indications include failed radiological control, recurrent bleeding, evidence of concomitant intraabdominal sepsis or lack of interventional radiology facilities [5]. When there are signs of delayed bleeding, early investigations and planned interventions (interventional radiology or surgery) result in definitive management and improved outcome.
| Materials and Methods | ▴Top |
This is a retrospective cohort study conducted in line with Strengthening the Reporting of Observational studies in Epidemiology (STROBE) guidelines after departmental approval at the University Hospitals Birmingham, United Kingdom, a tertiary center for pancreatic surgery [6]. Within a 12-year period (2011–2023) all patients that had any type of PD, classical or pylorus preserving, with or without vascular resection, were identified from a prospectively maintained database. Patients with signs of late postoperative hemorrhage (> 24 h) in the peritoneal cavity or in the GI tract, that underwent surgical or radiological intervention were included in the study. Patients that had suspected bleeding (e.g. hemoglobin drop, melaena, etc.) without any systemic response, transfusion requirement or radiological evidence of bleeding and did not require any intervention were excluded from the study. Investigations included computed tomography (CT) angiogram, invasive angiogram, routine blood tests, and upper GI endoscopy. Surgical intervention included suturing of bleeding vessel, packing and damage control surgery, and completion pancreatectomy. Endovascular treatment included embolization of pseudoaneurysm and stent graft insertion or both. Demographic, clinical biochemical, hematological, and radiological data were obtained from the hospital electronic records and the departmental prospectively maintained database.
Institutional Review Board (IRB) approval
This study was conducted as a retrospective cohort service evaluation at University Hospitals Birmingham NHS Foundation Trust and was reviewed according to local governance procedures. In line with UK Health Research Authority (HRA) guidance, it does not constitute research and did not require IRB approval.
Ethical compliance with human subjects
All procedures were conducted in accordance with institutional ethical standards for service evaluations and UK Health Research Authority guidance for studies that do not constitute research.
| Results | ▴Top |
A total of 1,184 PDs were performed between 2011 and 2023. Twenty-three (1.94%) patients had evidence of late PPH at a median of 15.6 (range 1–43) days (Table 1). In patients with evidence of post-operative pancreatic fistula (POPF), the median time to late PPH was 14 days. There were 18 male (78.3%) and five female patients (21.7%) with a median age of 62 years. Four patients (two male and two female) had a concomitant vascular resection. Fifteen (62.5%) patients had pancreatic fistula confirmed by biochemical test of drain fluid (fluid amylase > × 3 normal serum amylase) at the time of bleeding (Table 2).
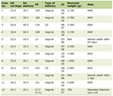 Click to view | Table 1. Patients’ Demographics, Intervention, and Outcome of Delayed Bleeding Post-PD |
Click to view | Table 2. Interval to Investigations for Patients With Delayed Bleeding After PD |
The majority of patients (20/23, 86.9%) had a systemic response following bleeding, identified by the National Early Warning Score (NEWS) assessment. Ten patients (43.5%) had bleeding in the surgical drain, and 13 patients (56.5%) had bleeding within the upper GI tract mostly evident with hematemesis or blood in the nasogastric tube. The majority of patients 20/23 (86.9%) had a CT angiogram within 12–24 h from the onset of bleeding.
Upper GI endoscopy, which was mainly diagnostic, was performed in two patients without clearly identifying any active bleeding point. No endoscopic interventions were performed in any of those patients.
Five patients (21.7%) underwent surgery and 18 (78.3%) endovascular treatment. Of those undergoing endovascular treatment, eight (34.8%) underwent coil embolization of an artery pseudoaneurysm, seven (30.4%) had a stent-graft placement, two (8.7%) had both embolization and stent graft, and one (4.3%) had a failed embolization. Of the patients who underwent surgery, two had oversewing of the gastroduodenal artery (GDA) stump, one had oversewing of the gastrojejunostomy suture line, one underwent general hemostasis with no obvious bleeding point identified, and one had bleeding from the pancreatic stump controlled.
The GDA was the location of bleeding in 10 patients (43.5%). Other areas included the right, left or common hepatic artery, the superior mesenteric artery (SMA), the left gastric artery, and splenic artery branches. In two patients, there was no obvious bleeding point identified in repeated imaging or invasive angiogram and in two patients the site of bleeding was early ulceration of the gastrojejunostomy. The in-hospital mortality rate was 17.4% (4/23), although one patient died due to causes unrelated directly to the bleeding episode, but bleeding contributed to an overall systemic deterioration.
Of the six patients in whom bleeding originated from the common hepatic artery and/or its branches, five demonstrated transient deterioration in hepatic function after interventional radiology which subsequently recovered in the days following successful intervention. More importantly, none of those developed any further liver-related complications.
One patient, who was initially discharged post-operatively, re-presented 4 weeks after pylorus-preserving pancreaticoduodenectomy (PPPD) with hematemesis. A CT angiogram demonstrated multiple collections surrounding the operative site, including a heterogeneous collection within the lesser sac concerning for internal hemorrhage, as well as locules of gas suggestive of an anastomotic leak at the pancreaticojejunostomy; however, no active bleeding source was identified on initial angiography. The patient continued to exhibit intraluminal bleeding over the subsequent 2 days and underwent repeat angiography, which identified the bleeding site and was treated with successful stent-graft placement. Despite this, the patient continued to deteriorate clinically, developed acute liver failure, and ultimately died in the intensive care unit (ICU) from multi-organ failure.
| Discussion | ▴Top |
Late bleeding, although rare, is a significant factor for increased morbidity and mortality after PD and is usually associated with evidence of pancreatic fistula and sepsis [7].
Three different grades of bleeding, A, B and C, are defined by the ISGPS according to the time of onset, location, actions required, and overall outcome, estimating a cumulative risk and clinical severity of the hemorrhage (Table 3) [8, 9]. The overall incidence of all grades of PPH varies from 3% to 29%, with a significantly increased mortality rate of 7–31% for grade C specifically [10]. The pathogenesis of late bleeding after PD is directly related to the complexity of surgery (extensive dissection and lymphadenectomy, vascular skeletonization and reconstruction, soft pancreas, and high-risk anastomosis), making vessels susceptible to bleeding due to local factors (e.g. pancreatic/biliary fistula, abscess) [11]. Several studies have investigated other independent risk factors that may predict late bleeding including high body mass index (BMI), younger age, prolonged operative time, intraoperative blood loss, and vascular reconstruction [12]. Interestingly those factors were also associated with an increased incidence of POPF, and the severity of bleeding was also associated with the degree of pancreatic fistula and its complications [3]. In one study, the presence of gas, rim enhancement, and isolation of candida species were identified as independent risk factors for late bleeding in patients with a pancreatic fistula and associated intrabdominal collection [13].
Click to view | Table 3. Proposed Classification of PPH: Clinical Condition, Diagnostic and Therapeutic Consequences |
It is important to identify the source and early signs of late bleeding and initiate the appropriate investigations and treatment. Approximately one-third of patients (28.2%) present with GI tract bleeding, whereas the rest have intra-abdominal hemorrhage as reported in one study [11].
Immediate CT angiography after appropriate resuscitation, when signs of bleeding occur or is suspected, regardless of severity and location, is strongly recommended. In our unit, we have a very low threshold for performing imaging and the majority of patients had a CT angiogram within 24 h after the onset of bleeding as shown in Table 1. Diagnostic and therapeutic endoscopy is an additional option and may be of value in controlling bleeding from a staple line or an early anastomotic ulcer but does not replace CT or formal angiogram to identify a pseudoaneurysm which must always be ruled out [11]. In fact, patients with pseudoaneurysms may remain asymptomatic without any evidence of bleeding. In one study, 27% of pseudoaneurysms were incidentally detected on routine CT imaging for other indications [3]. In our unit, we routinely perform a CT angiogram in all high-risk patients who have evidence of clinical or radiological pancreatic fistula before discharge even if they have no signs of bleeding to rule out an uncomplicated pseudoaneurysm. A meta-analysis of 14 studies reported the sensitivity of CT angiogram to identify the source of late bleeding to be only 67%. Sentinel bleed is also another scenario where CT may be initially negative [14]. Khalsa et al reported an overall sentinel bleed prevalence of 33% and found that this has been associated with a higher relaparotomy and mortality rate compared to late bleeding patients without a sentinel bleed episode [15].
Invasive angiogram offers both diagnostic and therapeutic options and can be considered when there is evidence of ongoing bleeding even with initially negative CT findings [16]. Angiography may be more sensitive and can identify hemorrhage when the bleeding rate is low (0.5 mL/min). Super-selective catheter placement may be required to maximize benefit [1]. Transcatheter arterial embolization has been widely accepted as the first-line treatment in the management of a bleeding pseudoaneurysm after PD and has a success rate of 67–100%, morbidity rate of 14–25%, and mortality rate of 0–14% [2, 16, 17]. Stent grafting is an alternative option instead of or in addition to embolization in selected patients. It offers the advantage of providing continued perfusion to the end-organ (e.g. liver) and may be useful in cases of a short stump or recurrent bleeding after previous embolization [17, 18]. Anatomical variations or acute arterial angulation may cause technical difficulties in the placement of the stent-graft. Routine post-procedure anticoagulation is not usually recommended [19].
Patients with ongoing bleeding but with radiologically negative findings to identify the source, may benefit from empiric embolization especially if they become systemically unstable. The GDA appears to be the most common site of bleeding (35–45%) in many studies [15]. In our series, the majority of bleeding was related to the GDA or SMA branches (47.8%). Yekebas et al reported a success rate of 80% in five patients who had empiric embolization of either GDA or SMA branches [20]. In our series, two patients were successfully treated with empiric GDA embolization or stenting (due to short stump).
Surgical management of bleeding is associated with higher mortality and morbidity compared to endovascular treatment [16]. This is possibly reflecting the fact that these patients: 1) often require urgent intervention due to severe bleeding and instability, 2) may have recurrent intractable bleeding with previous failed endovascular treatment, multiple transfusions, and coagulopathy, 3) may have high volume hemoperitoneum that would require washout, and 4) may have associated intrabdominal sepsis from pancreatic fistula and require control of both sepsis and bleeding [20]. In cases of failed endovascular treatment, the angiography performed at the time may still be helpful to identify the location of bleeding facilitating operative strategy [21]. In our study, 5/23 patients (21.7%) had surgical intervention all of them during the early part of the 12 years study period. Surgery may be very useful when bleeding is intraluminal (staple lines, early ulceration) and endoscopy fails to control. Various surgical techniques have been described aiming to prevent pseudoaneurysm formation intraoperatively including: 1) performing the pancreaticojejunostomy as far away as possible from the coeliac trunk and portal vein, or putting an omental flap around it, and 2) the use of the round ligament around the GDA stamp. The real benefits of these modifications remain at the level of local expertise [2, 4]. In a recent systematic review by Montorsi et al focusing in methods that can prevent and mitigate PHH, there were three randomized controlled trials (RCTs) identified that have proved to reduce the risk of PPH following specific surgical strategies including: 1) performing a smaller jejunal incision when creating the end to side duct to mucosa pancreaticojejunostomy, 2) creating a falciform ligament patch around the GDA or hepatic artery, and 3) performing a pancreaticojejunostomy instead of a pancreaticogastrostomy [22]. In our unit, when arterial resection and reconstruction is undertaken (e.g. hepatic artery), we perform total pancreatectomy to prevent pseudoaneurysm formation from possible pancreatic fistula.
The management of patients with recurrent bleeding after first treatment either surgery or interventional radiology remains challenging. The re-bleeding rate has been reported to be 28% after the first treatment in one study [1]. Possible causes include persistent surgical bed inflammation and infection from ongoing pancreatic leak, which can also cause new bleeding sites (28.6% of patients in one study), and failed endovascular treatment (coil migration, insufficient covered stent placement, endoleaks, recanalization of vessels) [14].
This study has several limitations. First, its retrospective design may introduce selection and information bias. In addition, the analysis relies primarily on descriptive statistics without inferential statistical testing, which limits the ability to identify independent predictors of late hemorrhage. Furthermore, other potentially relevant clinical variables, such as tumor characteristics, pancreatic texture, details of vascular resection or reconstruction, perioperative liver function, and management of pancreatic fistula prior to bleeding, were not systematically analyzed and may have influenced outcomes.
Conclusions
Late bleeding after PD commonly but not always is related to pancreatic leak. Early intervention after signs of bleeding results in the location of bleeding and potential definitive intervention. Endovascular treatment remains the most effective approach. When no source of bleeding can be identified, empiric embolization/stenting of the GDA provides an alternative option. Surgery may also be required in cases where ongoing sepsis causes recurrent bleeding episodes not amenable to endovascular treatment.
Acknowledgments
The authors thank the Clinical Audit and Service Evaluation Team at University Hospitals Birmingham NHS Foundation Trust for their support and facilitation of data access.
Financial Disclosure
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of Interest
The authors declare that there is no conflict of interest.
Informed Consent
Not applicable.
Author Contributions
Dobrzycka MA: data curation (lead); formal analysis (lead); project administration (lead); visualization (lead); investigation (lead); writing – review and editing (equal); final approval of manuscript (equal). Chatzizacharias N: writing – review and editing (supporting); final approval of manuscript (equal). Bisht H: data curation (supporting); investigation (supporting); writing – review and editing (supporting); final approval of manuscript (equal). Raza SS: writing – review and editing (supporting); final approval of manuscript (equal). Dasari BV: writing – review and editing (supporting); final approval of manuscript (equal). Bartlett DC: writing – review and editing (supporting); final approval of manuscript (equal). Marudanayagam R: writing – review and editing (supporting); final approval of manuscript (equal). Roberts KJ: writing – review and editing (supporting); final approval of manuscript (equal). Sutcliffe RP: writing – review and editing (supporting); final approval of manuscript (equal). Papamichail M: conceptualization (lead); methodology (lead); writing – original draft (lead); supervision (lead); writing – review and editing (equal); final approval of manuscript (equal).
Data Availability
The dataset used and analyzed during the current study is available from the corresponding author on reasonable request and with appropriate institutional approvals.
Abbreviations
BMI: body mass index; CT: computed tomography; GDA: gastroduodenal artery; GI: gastrointestinal; HRA: Health Research Authority; ICU: intensive care unit; IRB: Institutional Review Board; ISGPS: International Study Group of Pancreatic Surgery; NEWS: National Early Warning Score; PD: pancreaticoduodenectomy; PPH: pancreaticoduodenectomy hemorrhage; POPF: post-operative pancreatic fistula; RCT: randomized controlled trial; SMA: superior mesenteric artery; STROBE: Strengthening the Reporting of Observational Studies in Epidemiology
| References | ▴Top |
- Staerkle RF, Gundara JS, Hugh TJ, Maher R, Steinfort B, Samra JS. Management of recurrent bleeding after pancreatoduodenectomy. ANZ J Surg. 2018;88(5):E435-E439.
doi pubmed - Lee HG, Heo JS, Choi SH, Choi DW. Management of bleeding from pseudoaneurysms following pancreaticoduodenectomy. World J Gastroenterol. 2010;16(10):1239-1244.
doi pubmed - Chipaila J, Kato H, Iizawa Y, Motonori N, Noguchi D, Gyoten K, Hayasaki A, et al. Prolonged operating time is a significant perioperative risk factor for arterial pseudoaneurysm formation and patient death following hemorrhage after pancreaticoduodenectomy. Pancreatology. 2020;20(7):1540-1549.
doi pubmed - Roulin D, Cerantola Y, Demartines N, Schafer M. Systematic review of delayed postoperative hemorrhage after pancreatic resection. J Gastrointest Surg. 2011;15(6):1055-1062.
doi pubmed - Asari S, Matsumoto I, Toyama H, Yamaguchi M, Okada T, Shinzeki M, Goto T, et al. Recommendation of treatment strategy for postpancreatectomy hemorrhage: Lessons from a single-center experience in 35 patients. Pancreatology. 2016;16(3):454-463.
doi pubmed - von Elm E, Altman DG, Egger M, Pocock SJ, Gotzsche PC, Vandenbroucke JP, Initiative S. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. J Clin Epidemiol. 2008;61(4):344-349.
doi pubmed - Hur S, Yoon CJ, Kang SG, Dixon R, Han HS, Yoon YS, Cho JY. Transcatheter arterial embolization of gastroduodenal artery stump pseudoaneurysms after pancreaticoduodenectomy: safety and efficacy of two embolization techniques. J Vasc Interv Radiol. 2011;22(3):294-301.
doi pubmed - Wente MN, Veit JA, Bassi C, Dervenis C, Fingerhut A, Gouma DJ, Izbicki JR, et al. Postpancreatectomy hemorrhage (PPH): an International Study Group of Pancreatic Surgery (ISGPS) definition. Surgery. 2007;142(1):20-25.
doi pubmed - Correa-Gallego C, Brennan MF, D'Angelica MI, DeMatteo RP, Fong Y, Kingham TP, Jarnagin WR, et al. Contemporary experience with postpancreatectomy hemorrhage: results of 1,122 patients resected between 2006 and 2011. J Am Coll Surg. 2012;215(5):616-621.
doi pubmed - Ansari D, Tingstedt B, Lindell G, Keussen I, Ansari D, Andersson R. Hemorrhage after major pancreatic resection: incidence, risk factors, management, and outcome. Scand J Surg. 2017;106(1):47-53.
doi pubmed - Limongelli P, Khorsandi SE, Pai M, Jackson JE, Tait P, Tierris J, Habib NA, et al. Management of delayed postoperative hemorrhage after pancreaticoduodenectomy: a meta-analysis. Arch Surg. 2008;143(10):1001-1007; discussion 1007.
doi pubmed - Liang X, Shi LG, Hao J, Liu AA, Chen DL, Hu XG, Shao CH. Risk factors and managements of hemorrhage associated with pancreatic fistula after pancreaticoduodenectomy. Hepatobiliary Pancreat Dis Int. 2017;16(5):537-544.
doi pubmed - Birgin E, Hempel S, Reeg A, Oehme F, Schnizer A, Rink JS, Froelich MF, et al. Development and validation of a model for postpancreatectomy hemorrhage risk. JAMA Netw Open. 2023;6(12):e2346113.
doi pubmed - Lin YM, Lin EY, Tseng HS, Lee RC, Huang HE, Wang SE, Shyr YM, et al. Preventive covered stent placement at the gastroduodenal artery stump in angiogram-negative sentinel hemorrhage after pancreaticoduodenectomy. Abdom Radiol (NY). 2021;46(10):4995-5006.
doi pubmed - Khalsa BS, Imagawa DK, Chen JI, Dermirjian AN, Yim DB, Findeiss LK. Evolution in the treatment of delayed postpancreatectomy hemorrhage: surgery to interventional radiology. Pancreas. 2015;44(6):953-958.
doi pubmed - Hwang K, Lee JH, Hwang DW, Song KB, Kwon J, Gwon DI, Shin JH, et al. Clinical features and outcomes of endovascular treatment of latent pseudoaneurysmal bleeding after pancreaticoduodenectomy. ANZ J Surg. 2020;90(12):E148-E153.
doi pubmed - Gwon DI, Kim YH, Ko GY, Kim JW, Ko HK, Kim JH, Shin JH, et al. Vascular plug-assisted retrograde transvenous obliteration for the treatment of gastric varices and hepatic encephalopathy: a prospective multicenter study. J Vasc Interv Radiol. 2015;26(11):1589-1595.
doi pubmed - Izumi H, Yoshii H, Fujino R, Takeo S, Nomura E, Mukai M, Suda S, et al. Endovascular treatment of postoperative hemorrhage after pancreatectomy: a retrospective study. BMC Gastroenterol. 2023;23(1):379.
doi pubmed - You Y, Heo JS, Han IW, Shin SH, Shin SW, Park KB, Cho SK, et al. Long term clinical outcomes of portal vein stenting for symptomatic portal vein stenosis after pancreaticoduodenectomy. Medicine (Baltimore). 2021;100(39):e27264.
doi pubmed - Yekebas EF, Wolfram L, Cataldegirmen G, Habermann CR, Bogoevski D, Koenig AM, Kaifi J, et al. Postpancreatectomy hemorrhage: diagnosis and treatment: an analysis in 1669 consecutive pancreatic resections. Ann Surg. 2007;246(2):269-280.
doi pubmed - Wellner UF, Kulemann B, Lapshyn H, Hoeppner J, Sick O, Makowiec F, Bausch D, et al. Postpancreatectomy hemorrhage—incidence, treatment, and risk factors in over 1,000 pancreatic resections. J Gastrointest Surg. 2014;18(3):464-475.
doi pubmed - Montorsi RM, Zonderhuis BM, Daams F, Busch OR, Kazemier G, Marchegiani G, Malleo G, et al. Treatment strategies to prevent or mitigate the outcome of postpancreatectomy hemorrhage: a review of randomized trials. Int J Surg. 2024;110(10):6145-6154.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (CC BY 4.0), which permits unrestricted use, distribution, and reproduction in any medium, including commercial use, provided the original work is properly cited.
Journal of Current Surgery is published by Elmer Press Inc.