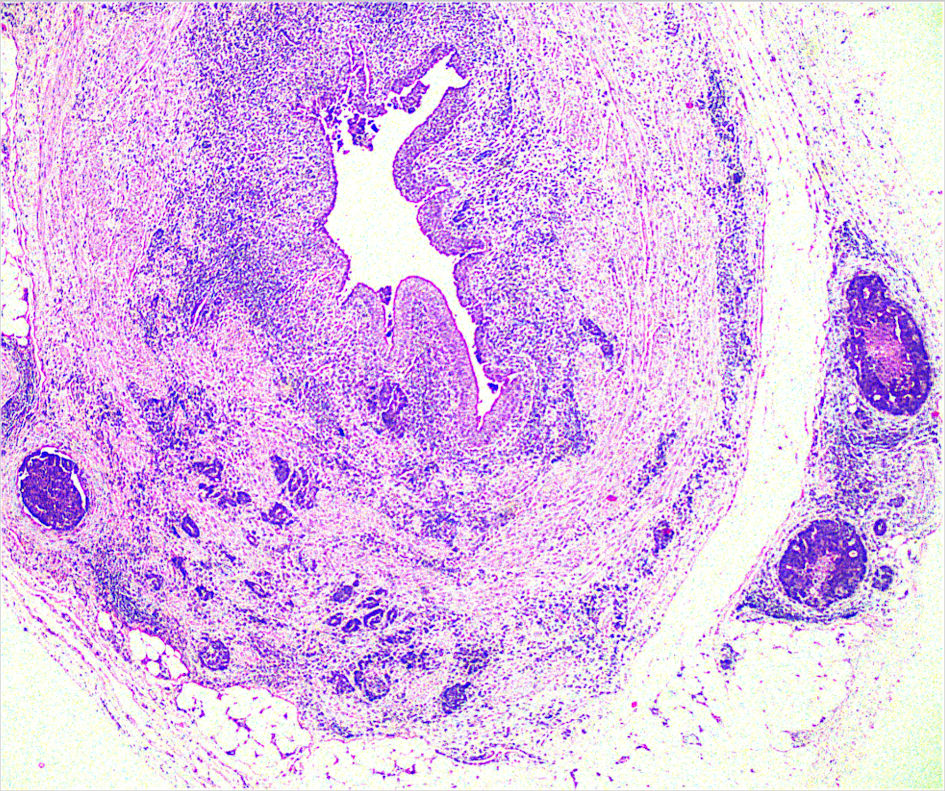
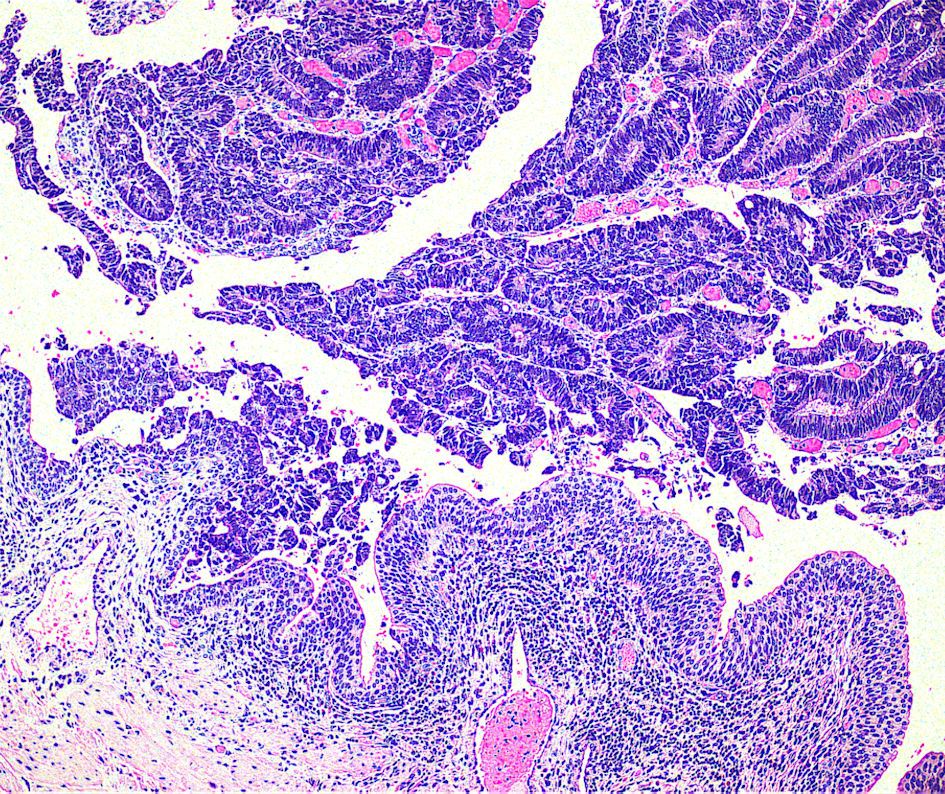
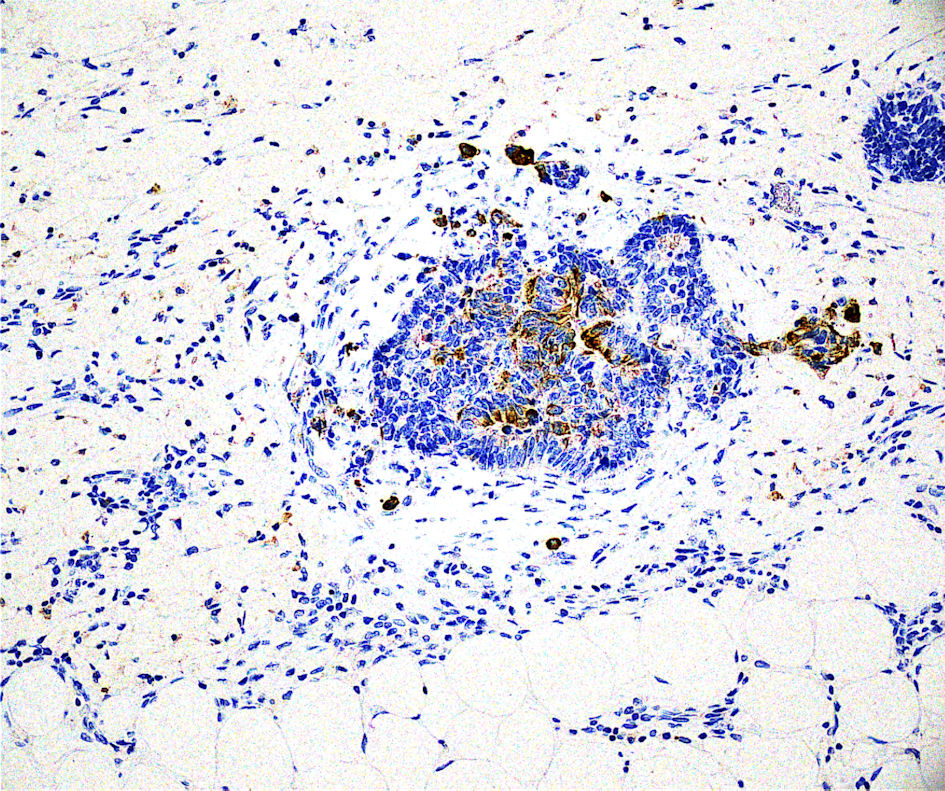
↓ Figure 1. Neoplastic aggregates in perirenal and periureteral fat with concurrent infiltration of all ureteral layers and papillary intraluminus morphology (× 200).
| Journal of Current Surgery, ISSN 1927-1298 print, 1927-1301 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Curr Surg and Elmer Press Inc |
| Journal website https://jcs.elmerpub.com |
Case Report
Volume 16, Number 1, June 2026, pages 16-19
Metastatic Sigmoid Adenocarcinoma at the Right Ureter
Figures
Table
| Months | Findings |
|---|---|
| CT: computed tomography; FOLFOX: folinic acid, 5-fluorouracil, oxaliplatin; MRI: magnetic resonance imaging; 18F-FDG PET-CT: 18F-fluorodeoxyglucose positron emission tomography–computed tomography; FOLFIRI: folinic acid, 5-fluorouracil, irinotecan. | |
| 0 | Urgent Hartmann’s sigmoidectomy, due to perforation of the underlying sigmoid colon adenocarcinoma (grade II, stage pT4aN2b), R0 resection |
| 1 | Staging: abdomen MRI and chest CT did not confirm metastatic lesions |
| 1–6 | Adjuvant chemotherapy with FOLFOX regimen |
| 6 | Follow-up abdomen MRI and chest CT, without evidence of recurrence or progression |
| 11 | Follow-up abdomen CT revealed abnormal lesion at the left ovary |
| 11 | Total hysterectomy with a bilateral salpingo-oophorectomy, which confirmed left ovary metastasis of the primary sigmoid adenocarcinoma, R0 resection |
| 13 | Examination with 18-FDG PET-CT, which showed abnormal para-aortic and iliac lymph nodes |
| 13–19 | First-line chemotherapy/immunotherapy with FOLFIRI/panitumumab regimen |
| 19 | Follow-up abdomen and chest CT, without evidence of recurrence or progression, and with radiographically complete response of the retroperitoneal lymphadenopathy |
| 24 | Follow-up abdomen and chest CT detected intraluminal lesions of the middle and lower third of the right ureter |
| 25 | Diagnostic right ureteroscopy confirmed the presence of papillary lesions totally obstructing the ureter |
| 26 | Right nephroureterectomy, with histopathological examination confirming metastatic adenocarcinoma of colon origin, R0 resection |