| Journal of Current Surgery, ISSN 1927-1298 print, 1927-1301 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Curr Surg and Elmer Press Inc |
| Journal website https://jcs.elmerpub.com |
Case Report
Volume 16, Number 1, June 2026, pages 16-19

Metastatic Sigmoid Adenocarcinoma at the Right Ureter
Nikolaos Giannirisa, c, Anastasia Therapontosb, Triantafyllos Papadopoulosa, Charalampos Kypraiosa, Ioannis Xoxakosa, Charikleia Kouvidoub, Ioannis Efthimioua
aDepartment of Urology, Evangelismos General Hospital of Athens, 10676 Athens, Greece
bDepartment of Pathology, Evangelismos General Hospital of Athens, 10676 Athens, Greece
cCorresponding Author: Nikolaos Gianniris, Department of Urology, Evangelismos General Hospital of Athens, 10676 Athens, Greece
Manuscript submitted January 28, 2026, accepted May 4, 2026, published online May 22, 2026
Short title: Metastatic Sigmoid Adenocarcinoma at the Ureter
doi: https://doi.org/10.14740/jcs1026
| Abstract | ▴Top |
Colorectal cancer and ureteral obstruction are both relatively common clinical entities. Although advancing carcinomas from neighboring organs can infiltrate and eventually block the ureter, distant ureteral metastasis from colon adenocarcinoma is a very rare condition. We present a case of a 68-year-old Caucasian female, with a right ureteral metastasis and a history of sigmoid cancer. The patient was referred to our department with asymptomatic moderate right hydronephrosis and hydroureter. She underwent right ureteroscopy, which revealed the abnormal tissue, and right nephroureterectomy. Histology showed infiltration of all layers of the ureteral wall, including the mucosa, by neoplastic cells with morphological and immunohistochemical features of colon adenocarcinoma. The patient was referred to the oncological department for oncological reevaluation.
Keywords: Colorectal cancer; Ureteral metastasis; Ureteral obstruction; Nephroureterectomy
| Introduction | ▴Top |
The obstruction of the ureter by direct invasion of retroperitoneal or pelvic tumors is relatively frequent. On the other hand, the development of a distant ureteral metastasis is an infrequent event, with only approximately 400 cases reported, from various primary tumors [1]. Distant ureteral metastases may occur via lymphatic and/or blood vessels [2, 3]. The criteria for establishing true ureteral metastasis from any cancer type, have been defined and consist of the following features: a clear distance between the primary tumor and metastasis, an identical cellularity of the two tumors, and the presence of malignant cells in the vascular and lymphatic system of the ureteral wall [2, 3]. Primary tumors have been described as these of the breast, colon, rectum, stomach, lung, cervix, prostate, pancreas, and lymphoma [3–5]. We present a case of distant ureteral metastasis from sigmoid adenocarcinoma, which is considered to be very rare [1–6].
| Case Report | ▴Top |
A 66-year-old Caucasian female with no medical history presented to the emergency department with a clinical presentation of acute abdomen, due to sigmoid colon perforation. She was admitted to the hospital and underwent urgent Hartmann’s sigmoidectomy, with the formation of an end colostomy. The histological examination revealed sigmoid colon adenocarcinoma (grade II, stage pT4aN2b), with tumor infiltration in 13 of the 20 resected lymph nodes, and R0 surgical margins. The microsatellite instability and mismatch repair genes mutation tests, as well as the Kirsten rat sarcoma virus oncogene homologue (KRAS), neuroblastoma rat sarcoma virus oncogene homologue (NRAS) and v-raf murine sarcoma viral oncogene homolog B1 (BRAF) gene mutation tests proved negative for the aforementioned adenocarcinoma. Magnetic resonance imaging (MRI) examination of the abdomen and computed tomography (CT) examination of the chest, after the surgery, did not confirm metastatic lesions. Biomarkers carcinoembryonic antigen (CEA) and carbohydrate antigen 19-9 (CA19-9) levels were not elevated at first diagnosis or during routine biochemical follow-up.
The patient was then referred to the oncological department and received adjuvant chemotherapy with folinic acid, 5-fluorouracil, oxaliplatin (FOLFOX) regimen, which was completed 6 months after the emergency sigmoidectomy. At the same time, she was subjected to follow-up examinations with abdomen MRI and chest CT.
During subsequent follow-up, an abnormal pelvic mass at the position of the left ovary was identified. Eleven months after the first surgery, the patient underwent resection of this pelvic mass, along with total hysterectomy with a bilateral salpingo-oophorectomy. The pathological examination confirmed left ovary metastasis of the primary sigmoid adenocarcinoma, with an R0 resection, and negative KRAS, NRAS and BRAF gene mutation tests. 18F-fluorodeoxyglucose positron emission tomography–computed tomography ((18F)-FDG PET-CT) performed 2 months after the second surgery (pelvic mass resection) showed abnormal para-aortic and iliac lymph nodes. Consequently, following oncological evaluation, the patient was introduced to first-line chemotherapy/immunotherapy with folinic acid, 5-fluorouracil, irinotecan (FOLFIRI)/panitumumab regimen, which was completed 19 months after the first surgery (sigmoidectomy). At that time, there was radiographically complete response of the retroperitoneal lymphadenopathy.
The patient remained free of recurrent disease for the following 5 months. During follow-up, CT of the abdomen detected intraluminal lesions of the middle and lower third of the right ureter, which manifested as right moderate hydronephrosis and hydroureter. The patient had no symptoms and normal renal function. Right ureteroscopy confirmed the presence of papillary lesions in the middle and lower third of the right ureter, totally obstructing it, while urine cytology was negative for malignant cells. Twenty-six months after the resection of the primary tumor (urgent sigmoidectomy due to perforation), following discussion in the hospital multidisciplinary tumor board, the patient was subjected to right nephroureterectomy. No post-nephroureterectomy complications were observed, and the renal function remained normal. The patient recovered and was discharged without any unexpected events.
The histology identified solid and cribriform neoplastic aggregates with focal comedo necrosis involving the perirenal and periureteral fat, with concurrent infiltration of the serosa/adventitia, muscular layer, and mucosa of the ureter. In the latter, the neoplasm showed a papillary morphology consistent with ureteroscopy findings (Figs. 1, 2).
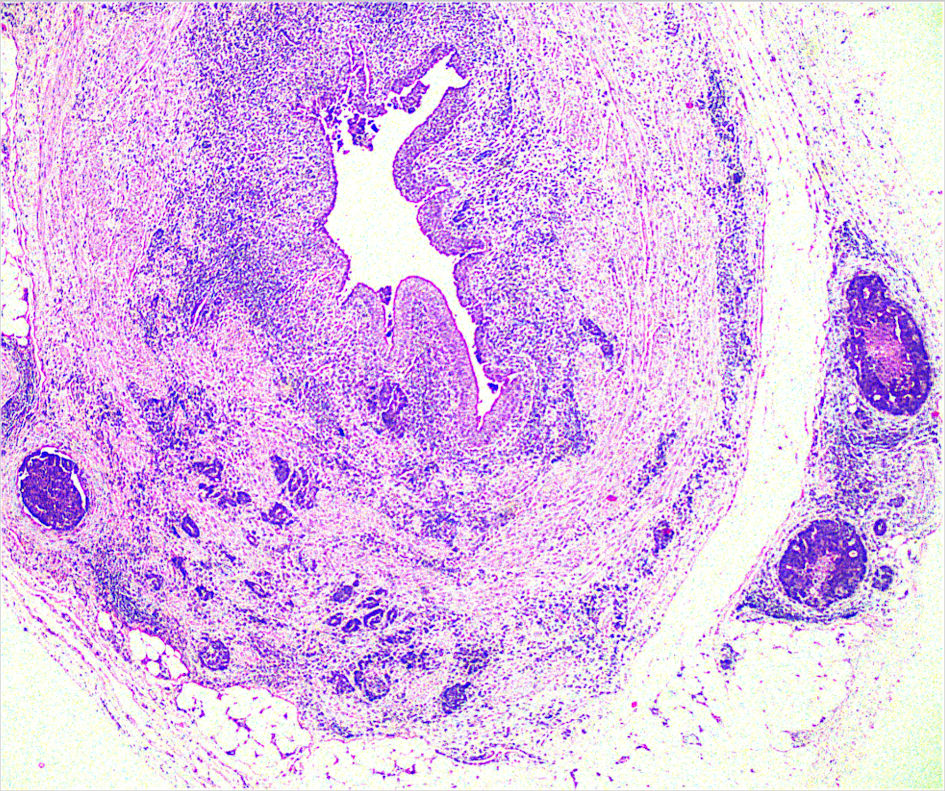 Click for large image | Figure 1. Neoplastic aggregates in perirenal and periureteral fat with concurrent infiltration of all ureteral layers and papillary intraluminus morphology (× 200). |
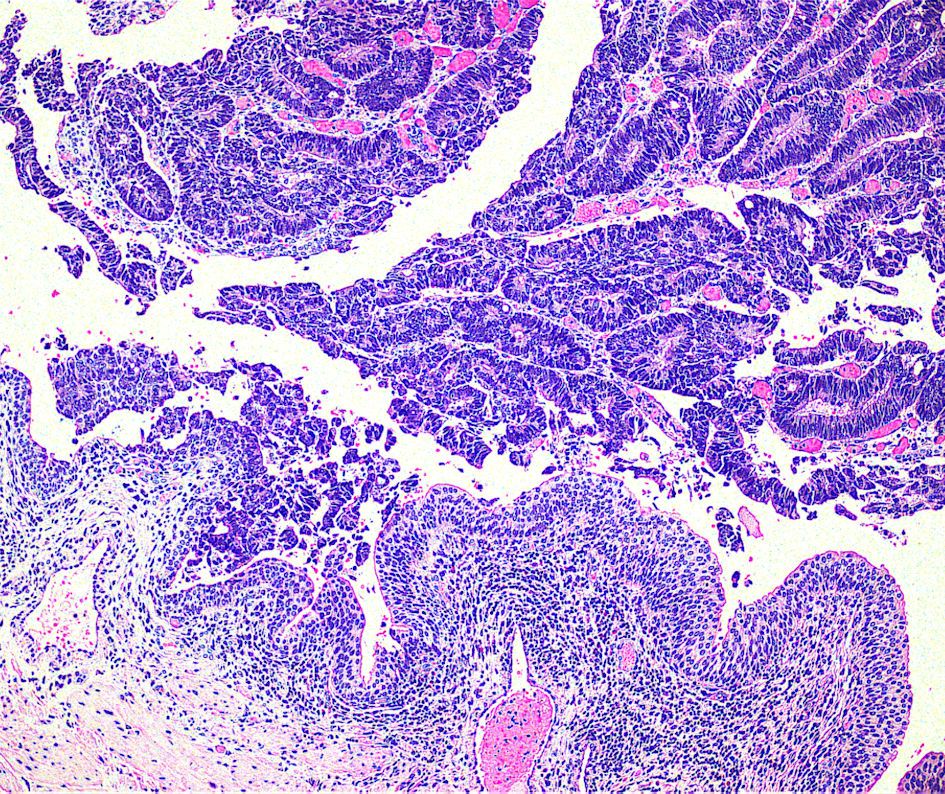 Click for large image | Figure 2. Solid and cribriform neoplastic aggregates focally with comedo necrosis (× 100). |
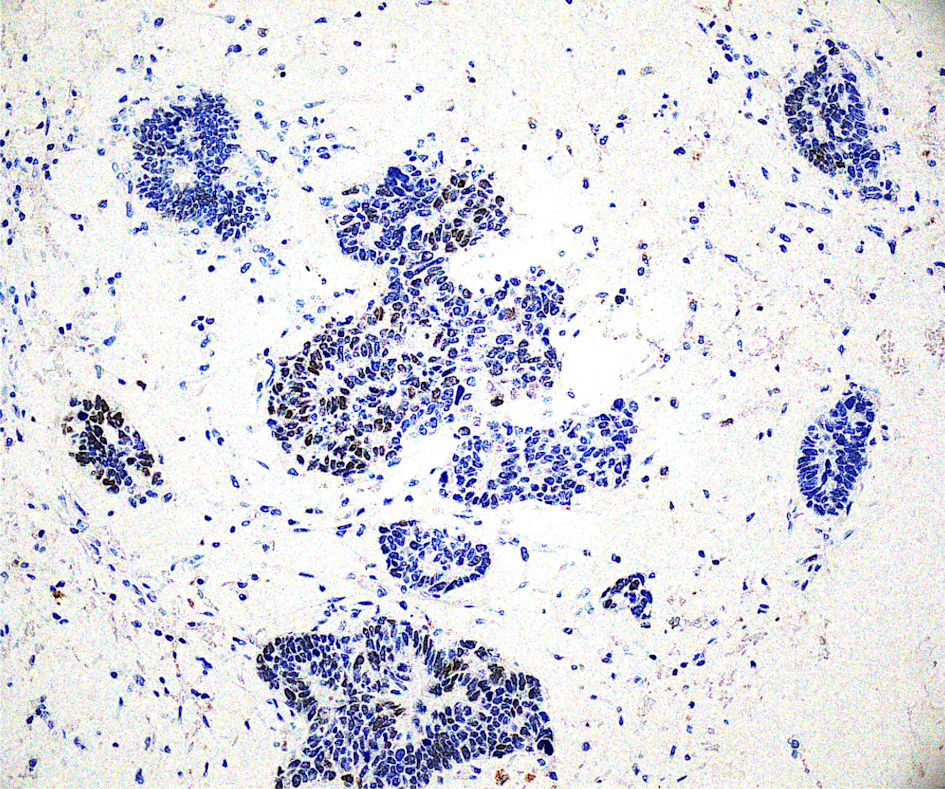
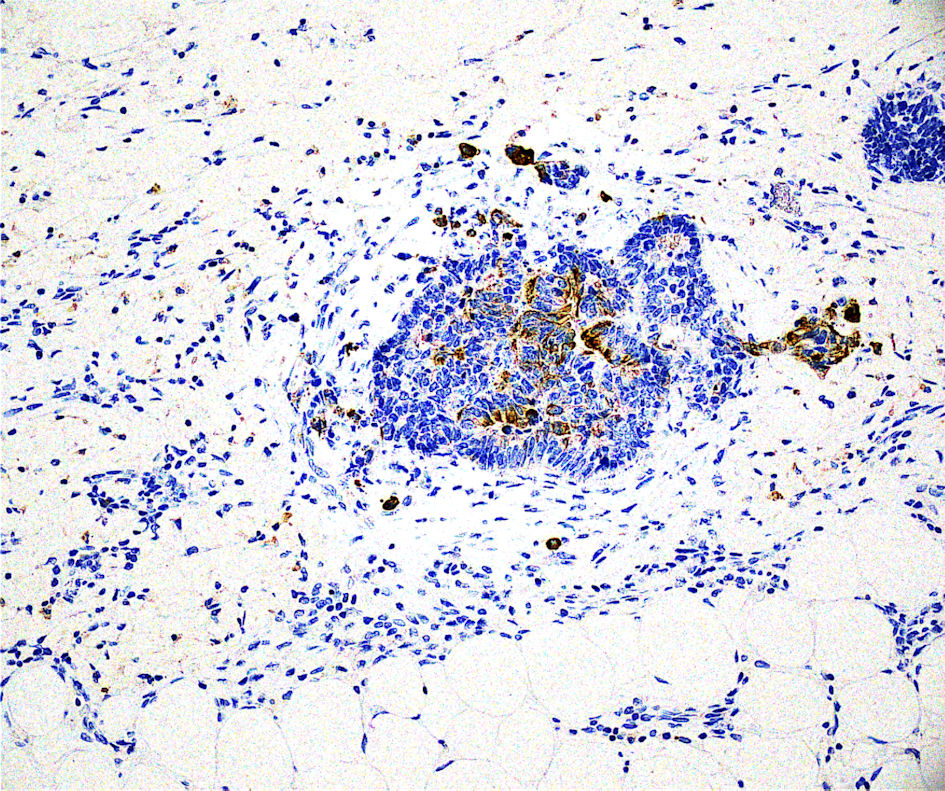
The immunohistochemistry profile of the neoplasm showed caudal-type homeobox 2 (CDX-2) (+), special adenine-thymine-rich sequence-binding protein 2 (SATB2) (+), cytokeratin 20 (CK20) (+, focal), cytokeratin 7 (CK7) (–), guanine-adenine-thymine-adenine-binding protein 3 (GATA3) (–), consistent with an adenocarcinoma of colon origin according to clinical history (Figs. 3–5).
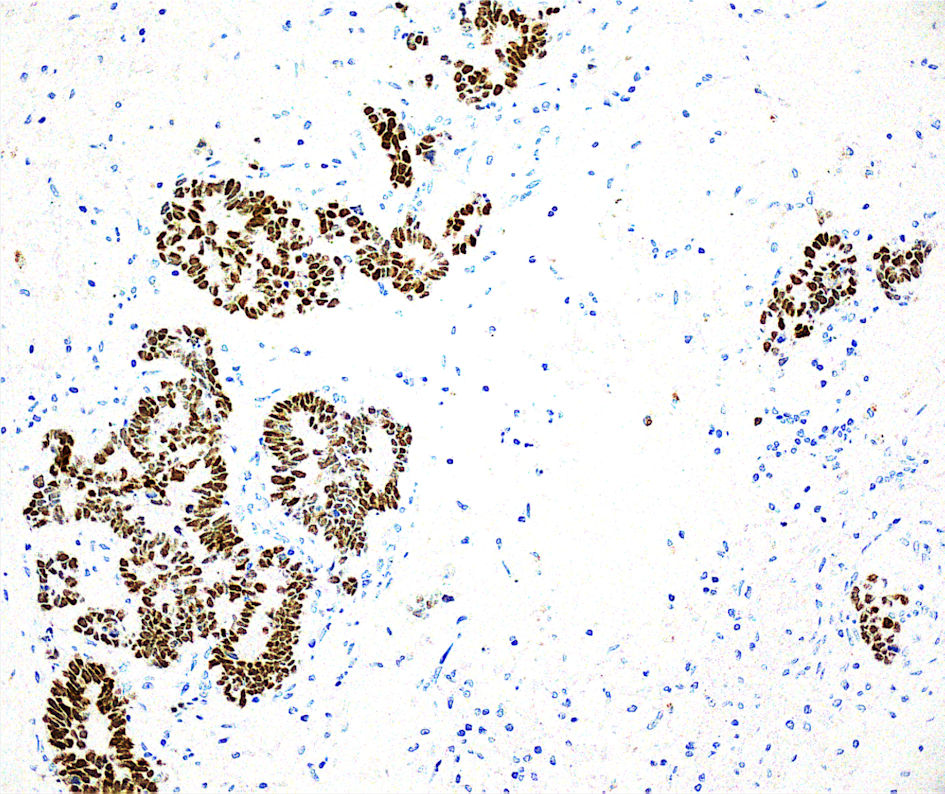 Click for large image | Figure 3. Immunohistochemistry profiling, CDX-2 positive (× 200). CDX2: caudal-type homeobox 2. |
 Click for large image | Figure 4. Immunohistochemistry profiling, SATB2 positive (× 200). SATB2: special adenine-thymine-rich sequence-binding protein 2. |
 Click for large image | Figure 5. Immunohistochemistry profiling, CK20 positive (focal, × 200). CK20: cytokeratin 20. |
Following these findings, the patient was referred to the oncological department for oncological reevaluation (Table 1).
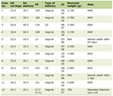 Click to view | Table 1. Patient Timeline |
| Discussion | ▴Top |
A considerable number of colorectal cancer patients develop distant metastases [7]. Distant ureteral metastasis from primary colon adenocarcinoma is very rare and was first reported in 1936 [2]. Hu et al conducted a systematic review of ureteral involvement by metastatic malignant disease, which identified 265 cases with various cancer metastasis to the ureter. The most common sites of primary tumor included the prostate, bladder, breast, intestines, and lymphoma. Only 35 of the 265 cases involved ureteral metastasis from a small or large intestine primary cancer. In this analysis, metastatic ureteral cancer from an intestinal primary was diagnosed at an average of 24 months after diagnosis of the primary lesion, which is consistent with our case [6].
There are three different types of metastatic cancer involvement of the ureter [4, 5, 8, 9]: 1) Type I—periureteral adventitial layer infiltration by the malignant cells, the most common one of the three types, usually resulting in compression of the ureter; 2) Type II—partial involvement of the layers of the ureteral wall, with presence of tumor cells in the muscular layer and/or transmural lymphatic/vascular involvement; 3) Type III— involvement of ureteral mucosa, with or without muscular layer, often presenting as submucosal nodules and representing the most uncommon.
Type I and type II result in ureteral stricture formation and may even cause obstruction of the ureter with or without associated mass. Type III may manifest as intraluminal lesions seen radiographically, such as in our case [9].
According to publish data, as in our patient, the metastatic involvement of ureter is usually asymptomatic. Surgeons should receive a high index of suspicion of ureteral metastasis when hydronephrosis is identified during follow-up [10, 11].
Metastatic colon adenocarcinoma at the ureter has an aggressive progression and a poor prognosis, as depicted by the unfavorable long-term survival evidence of the few reported cases. Distinguishing primary carcinoma of the urinary tract from metastatic adenocarcinoma is essential for excellent patient care and therapy schedule. There are no standardized treatment protocols, since it constitutes a very rare condition, but chemotherapy in combination with surgical treatment forms a reasonable option [3–6, 12]. There is evidence indicating that patients who underwent surgery had better outcomes [6], which demonstrates that ureteral colon cancer metastasectomy follows the evidence of liver and lung metastasectomy from colon cancer, which improves prognosis.
Conclusions
Metastatic colon adenocarcinoma at the ureter is rarely encountered in clinical practice. However, it should be considered in the differential diagnosis, once there is clinical or radiographic evidence of ureteral obstruction in a patient, who has a history of colon cancer, regardless of the stage and previous therapy.
Acknowledgments
None to declare.
Financial Disclosure
No funding was received in regard to the production of this paper.
Conflict of Interest
The authors declare that there is no conflict of interest regarding the publication of this paper.
Informed Consent
Informed consent was obtained from the patient for publication of this case report.
Author Contributions
Dr. Nikolaos Gianniris: conceptualization, literature review, data collection, data analysis, original manuscript drafting, visualization. Dr. Anastasia Therapontos: literature review, data collection, data analysis. Dr. Triantafyllos Papadopoulos: literature review, data collection, data analysis. Dr. Charalampos Kypraios: literature review, data collection, data analysis. Dr. Ioannis Xoxakos: literature review, data collection, data analysis. Dr. Charikleia Kouvidou: literature review, data collection, data analysis, manuscript review and editing. Dr. Ioannis Efthimiou: literature review, data collection, data analysis, manuscript review and editing.
Data Availability
All relevant data supporting the findings of this case report are included in the manuscript.
Abbreviations
KRAS: Kirsten rat sarcoma virus oncogene homologue; NRAS: neuroblastoma rat sarcoma virus oncogene homologue; BRAF: v-raf murine sarcoma viral oncogene homolog B1; CT: computed tomography; CEA: carcinoembryonic antigen; CA19-9: carbohydrate antigen 19-9; FOLFOX: folinic acid, 5-fluorouracil, oxaliplatin; MRI: magnetic resonance imaging; 18F-FDG PET-CT: 18F-fluorodeoxyglucose positron emission tomography–computed tomography; FOLFIRI: folinic acid, 5-fluorouracil, irinotecan; CDX-2: caudal-type homeobox 2; SATB2: special adenine-thymine-rich sequence-binding protein 2; CK20: cytokeratin 20; CK7: cytokeratin 7; GATA3: guanine-adenine-thymine-adenine-binding protein 3
| References | ▴Top |
- Haddad FS. Metastases to the ureter. Review of the world literature, and three new case reports. J Med Liban. 1999;47(4):265-271.
pubmed - Mackenzie DW, Ratner M. Metastatic growths in the ureter: a report of three cases and a brief review of the literature. Can Med Assoc J. 1931;25(3):265-270.
pubmed - Presman D, Ehrlich L. Metastatic tumors of the ureter. J Urol. 1948;59(3):312-325.
doi pubmed - Cohen WM, Freed SZ, Hasson J. Metastatic cancer to the ureter: a review of the literature and case presentations. J Urol. 1974;112(2):188-189.
doi pubmed - Fitch WP, Robinson JR, Radwin HW. Metastatic carcinoma of the ureter. Arch Surg. 1976;111(8):874-876.
doi pubmed - Hu J, Deng J, Guo J, Fu B. Ureteral involvement by metastatic malignant disease. Clin Exp Metastasis. 2019;36(6):499-509.
doi pubmed - Aran V, Victorino AP, Thuler LC, Ferreira CG. Colorectal cancer: epidemiology, disease mechanisms and interventions to reduce onset and mortality. Clin Colorectal Cancer. 2016;15(3):195-203.
doi pubmed - Marincek B, Scheidegger JR, Studer UE, Kraft R. Metastatic disease of the ureter: patterns of tumor spread and radiologic findings. Abdominal Imaging. 1993;18:88-94.
- Arvind NK, Singh O, Gupta S, Ali Q. Ureteral metastasis as the presenting manifestation of pancreatic carcinoma. Rev Urol. 2013;15(3):124-130.
pubmed - Loloi J, Kuan K, Cheng J, Kovac E, Aboumohamed A. Ureteral metastasis in colorectal cancer: a case report and review of literature. Urol Case Rep. 2021;39:101851.
doi pubmed - Moynihan MJ, Moinzadeh A, Mandeville JA. Symptomatic ureteral metastasis from colon adenocarcinoma. J Endourol Case Rep. 2020;6(2):80-82.
doi pubmed - Dickson BC, Fornasier VL, Streutker CJ, Stewart RJ. Ureteric obstruction: an unusual presentation of metastatic colon carcinoma. Can J Urol. 2007;14(2):3526-3528.
pubmed
This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (CC BY 4.0), which permits unrestricted use, distribution, and reproduction in any medium, including commercial use, provided the original work is properly cited.
Journal of Current Surgery is published by Elmer Press Inc.