| Journal of Current Surgery, ISSN 1927-1298 print, 1927-1301 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Curr Surg and Elmer Press Inc |
| Journal website https://jcs.elmerpub.com |
Original Article
Volume 16, Number 1, June 2026, pages 9-15

The Necessity of Surgical Intervention in Acute Intracerebral Hematomas
Hakan Aka, c ![]() , Sedanur Ozgulb
, Sedanur Ozgulb ![]() , Emine Avginb
, Emine Avginb ![]()
aDepartment of Neurosurgery, School of Medicine, Kirsehir Ahi Evran University, Kirsehir, Turkiye
bKirsehir Training and Research Hospital, Kirsehir, Turkiye
cCorresponding Author: Hakan Ak, Department of Neurosurgery, School of Medicine, Kirsehir Ahi Evran University, Kirsehir, Turkiye
Manuscript submitted March 16, 2026, accepted April 27, 2026, published online May 22, 2026
Short title: Surgery of Intracerebral Hematomas
doi: https://doi.org/10.14740/jcs1030
| Abstract | ▴Top |
Background: Spontaneous intracerebral hematoma (ICH) is a major cause of hemorrhagic stroke and is associated with high morbidity and mortality. Despite advances in neuroimaging, surgical techniques, and intensive care management, the optimal treatment strategy remains controversial. This study aimed to evaluate the demographic characteristics, hemorrhage features, underlying etiological factors, and clinical outcomes of patients who underwent surgical treatment for spontaneous ICH.
Methods: This descriptive study included patients with acute non-traumatic ICHs who were surgically treated between 2021 and 2025. Data regarding age, sex, comorbidities, use of anticoagulant or antiplatelet/fibrinolytic agents, pre- and postoperative Glasgow Coma Scale (GCS) scores, hemorrhage location and volume, ventricular involvement, surgical approach, and survival were retrospectively analyzed. Hematoma volume was calculated using the ABC/2 method.
Results: A total of 52 patients were included. Hematoma evacuation via craniotomy was performed in 26 patients (55.31%), external ventricular drainage (EVD) in 21 patients (44.69%), and both procedures in five patients. The overall first-month mortality rate was 46.80%. The majority of patients (95.74%) had at least one chronic comorbidity, and 82.97% were receiving anticoagulant and/or antiplatelet/fibrinolytic therapy. Patients undergoing craniotomy had large hematoma volumes (45–150 cm3) and low preoperative GCS scores (median: 5). In the EVD group, the first-month mortality rate was 47.61%.
Conclusion: Spontaneous ICHs are frequently associated with antithrombotic therapy and multiple comorbidities. Despite persistently high mortality and morbidity—particularly in patients with low GCS scores, large hematoma volumes, and intraventricular hemorrhage—surgical intervention remains an important option, offering selected patients a chance of survival and protecting physicians from medicolegal problems. Careful patient selection and optimal intensive care management are critical determinants of outcome.
Keywords: Intracerebral hemorrhage; Craniotomy; External ventricular drainage; Intraventricular hemorrhage; Glasgow Coma Scale; Surgical outcome
| Introduction | ▴Top |
As is well established, strokes are classified into ischemic and hemorrhagic types, with spontaneous intracerebral hematomas (ICHs) accounting for a substantial proportion of hemorrhagic strokes. This condition is characterized by a rapidly expanding hematoma within the brain parenchyma, with potential extension into the ventricular system as well as the subarachnoid and dural spaces. Globally, it is estimated to affect approximately 2 million individuals annually [1–4]. These hematomas are associated with high rates of morbidity and mortality. Reported mortality rates within the first month range between 30% and 50% [3–6]. Survivors, on the other hand, remain at high risk for long-term disabilities of varying severity, recurrent intracerebral hemorrhage, other serious vascular events, epilepsy, and neurological complications such as dementia [7]. In such types of hemorrhage, multiple underlying risk factors and associated diseases may be present.
Rapidly progressive neurological signs and symptoms, including headache, vomiting, seizures, and a level of impaired consciousness disproportionate to focal neurological deficits, should raise suspicion for an ICH. In such patients, prompt diagnostic evaluation is essential, and the location and size of the hemorrhage must be determined radiologically without delay. Therefore, computed tomography (CT) or magnetic resonance imaging (MRI) should be performed as first-line imaging modalities to differentiate intracerebral hemorrhage from acute ischemic stroke, as well as from hemorrhage-prone tumors or metastatic lesion [3, 6–8]. The optimal management of these hemorrhages remains controversial, with an ongoing debate between conservative management and surgical intervention. Conflicting results have been reported across different clinical studies. Various surgical techniques have been described, including decompressive craniectomy, craniotomy, external ventricular drainage (EVD), several minimally invasive approaches, and endoscopic procedures [6, 7, 9–11].
The present study aimed to comprehensively evaluate patients who underwent surgical treatment in our clinic. Specifically, we assessed their demographic characteristics, the location and volume of the hemorrhages, potential underlying etiological factors contributing to the bleeding, and the clinical outcomes following surgery. By systematically analyzing these variables, we sought to provide insights into the factors influencing surgical decision-making and patient prognosis.
| Materials and Methods | ▴Top |
The study included patients with acute non-traumatic ICHs who were treated at Kirsehir Training and Research Hospital between 2021 and 2025. In addition to demographic data such as age and sex, information was collected on comorbidities, preoperative Glasgow Coma Scale (GCS) scores, hemorrhage location, involvement of cerebral parenchyma and/or ventricular system, hemorrhage volume, surgical approach, and postoperative survival. Hemorrhage volume was calculated from CT images using the ABC/2 method [12]. In patients with isolated intraventricular hemorrhage, hemorrhage volume was not measured. Surgical intervention was performed based on changes in GCS scores and the development of hydrocephalus. Patients with abnormal bleeding parameters or a history of anticoagulant use not detectable by laboratory tests underwent surgery only after appropriate precautions were taken or after correction of the bleeding parameters. The study population consisted of patients presenting from the emergency department or those under follow-up who experienced a progressive decline in GCS scores, as well as patients who had suffered an ischemic cerebrovascular accident and subsequently developed hemorrhage after thrombolytic therapy, resulting in a significant drop, at least 2 points, in GCS.
For patients with cerebral parenchymal hemorrhages, a wide craniotomy was performed using a trauma flap incision. During craniotomy, the sphenoid wing was drilled and the temporal bone was excised up to the zygomatic arch to allow adequate decompression of the uncus. The hematoma was evacuated via corticotomy at the site closest to the hemorrhage. After hematoma evacuation, in patients where feasible, the dura was loosely closed using either primary closure or duraplasty. The bone flap was either replaced or, in some patients, implanted in the abdominal wall. EVD was applied only to patients with isolated ventricular hemorrhage or significant ventricular involvement. Patients with only cerebral parenchymal hemorrhage did not receive EVD. Cases with incomplete data, traumatic hemorrhages, and patients under 18 years of age were excluded from the study. Patients with a follow-up period shorter than 3 months or those managed conservatively without surgical intervention were also excluded.
This was a descriptive study, and data were presented as counts and percentages. For numerical variables, depending on their distribution, mean ± standard deviation (SD) or median with interquartile range (IQR) was reported.
Ethical compliance
Permission to conduct the study was obtained from the Kirsehir Provincial Health Directorate, dated January 21, 2026 and numbered E-72254678-770-302307852.
| Results | ▴Top |
A total of 52 patients were included in the study. Of these, 26 patients (55.31%) underwent hematoma evacuation via craniotomy, while 21 patients (44.69%) received EVD. It was determined that five patients underwent both craniotomy and EVD. Among all patients, 31 were female (65.95%) and 16 were male (34.05%). The follow-up period ranged from 4 to 52 months. In the EVD group, due to various reasons—such as EVD obstruction or the need for prolonged EVD placement exceeding 10 days to prevent colonization—EVD replacement was performed once in four patients and twice in two patients. In the craniotomy group, three patients required reoperation due to rebleeding.
The craniotomy/craniectomy group consisted of a total of 26 patients (n = 26). The age of the patients ranged from 31 to 80 years, with a mean age of 63.4 years (95% confidence interval (CI): 58.5–68.2; SD: 12.1). Of the patients, 69.2% were female (n = 18) and 30.8% were male (n = 8). While 23.1% of the patients (n = 6) were receiving anticoagulant therapy, 53.8% (n = 14) were using antiplatelet or fibrinolytic agents. Six patients were not using any anticoagulant, antiplatelet, or fibrinolytic medications. Except for one patient, all had various comorbid chronic conditions, including hypertension, diabetes mellitus, asthma, thyroid disease, chronic obstructive pulmonary disease, hypercholesterolemia, atrial fibrillation, coronary artery disease, mitral valve prolapse, chronic heart failure, a history of ischemic and/or hemorrhagic cerebrovascular disease, Wegener’s granulomatosis (in two patients), cardiac pacemaker implantation, epilepsy, dementia, benign prostatic hyperplasia, and malignancies such as brain, colon, breast, and lung cancer. Hemorrhage was right-sided in 31.8% of the patients. Based on volumetric measurements obtained from brain CT scans, hematoma volume ranged from 45 to 150 cm3, with a mean volume of 86 cm3 (median: 58 cm3). The median preoperative GCS score was 5 (range: 3–8), while the median early postoperative (first 6 h) GCS score was 6 (range: 3–12; IQR = 9). Within the first postoperative month, 12 patients died (46.15%), and of the remaining 14 patients, seven died within the first 3 months due to various causes. Among the remaining seven patients, three survived with moderate-to-severe disability, whereas four were able to live independently without assistance. The longest follow-up duration in this group was 52 months. Figures 1 and 2 illustrate CT images of representative cases from our series.
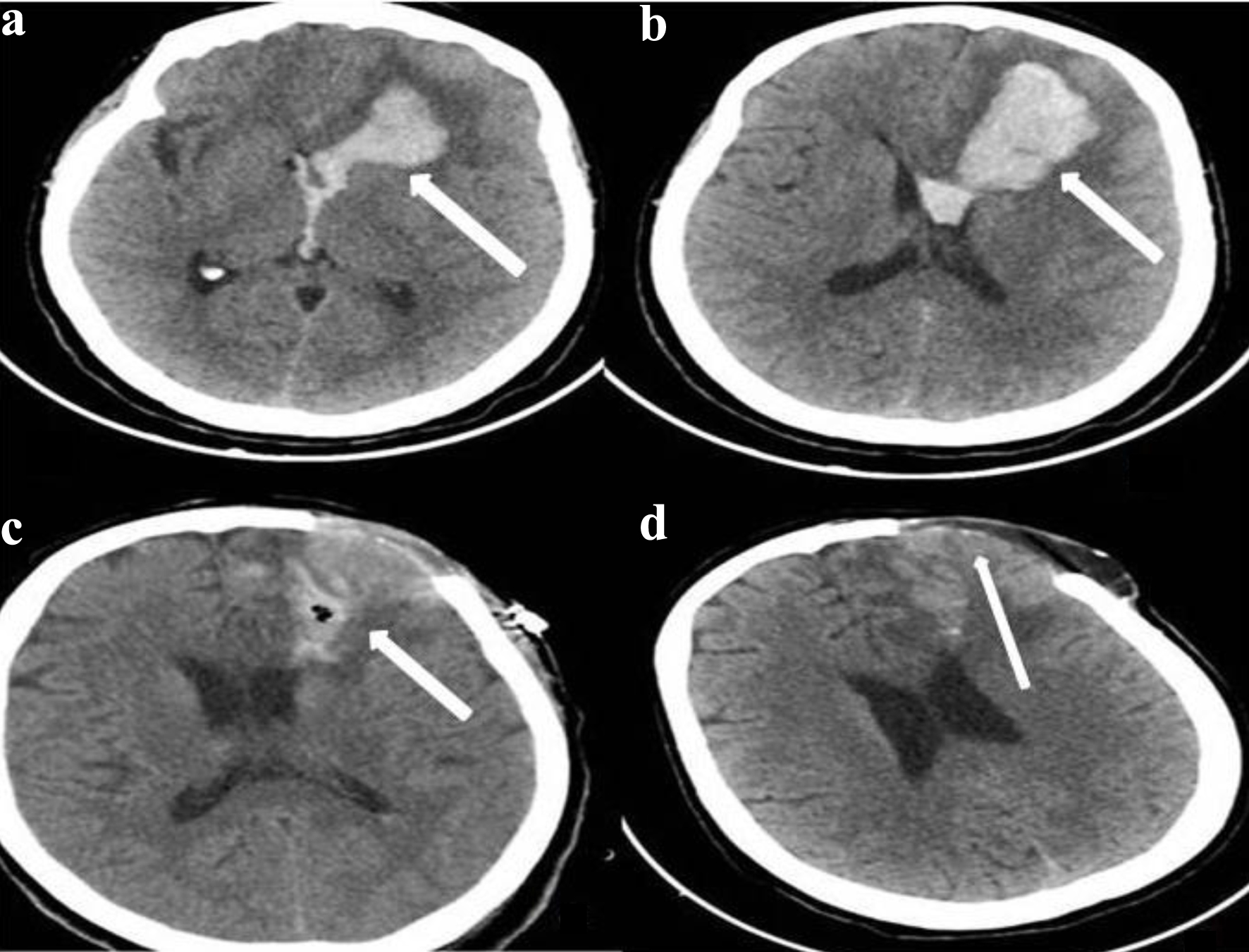 Click for large image | Figure 1. Axial brain computed tomography (CT) sections with a slice thickness of 2.5 mm. Images (a) and (b) are preoperative scans demonstrating hyperdense hemorrhagic areas in the left frontal region with extension into the ventricle (the white arrow indicates the hemorrhage). Image (c) is a 2.5-mm axial CT scan obtained in the early postoperative period, 3 days after surgery (the white arrow indicates early postoperative changes at the surgical site). Image (d) is a 2.5-mm axial CT scan obtained 1 month after surgery, showing no evidence of hemorrhage (the white arrow indicates the previous hemorrhage evacuation site and the bone defect area). |
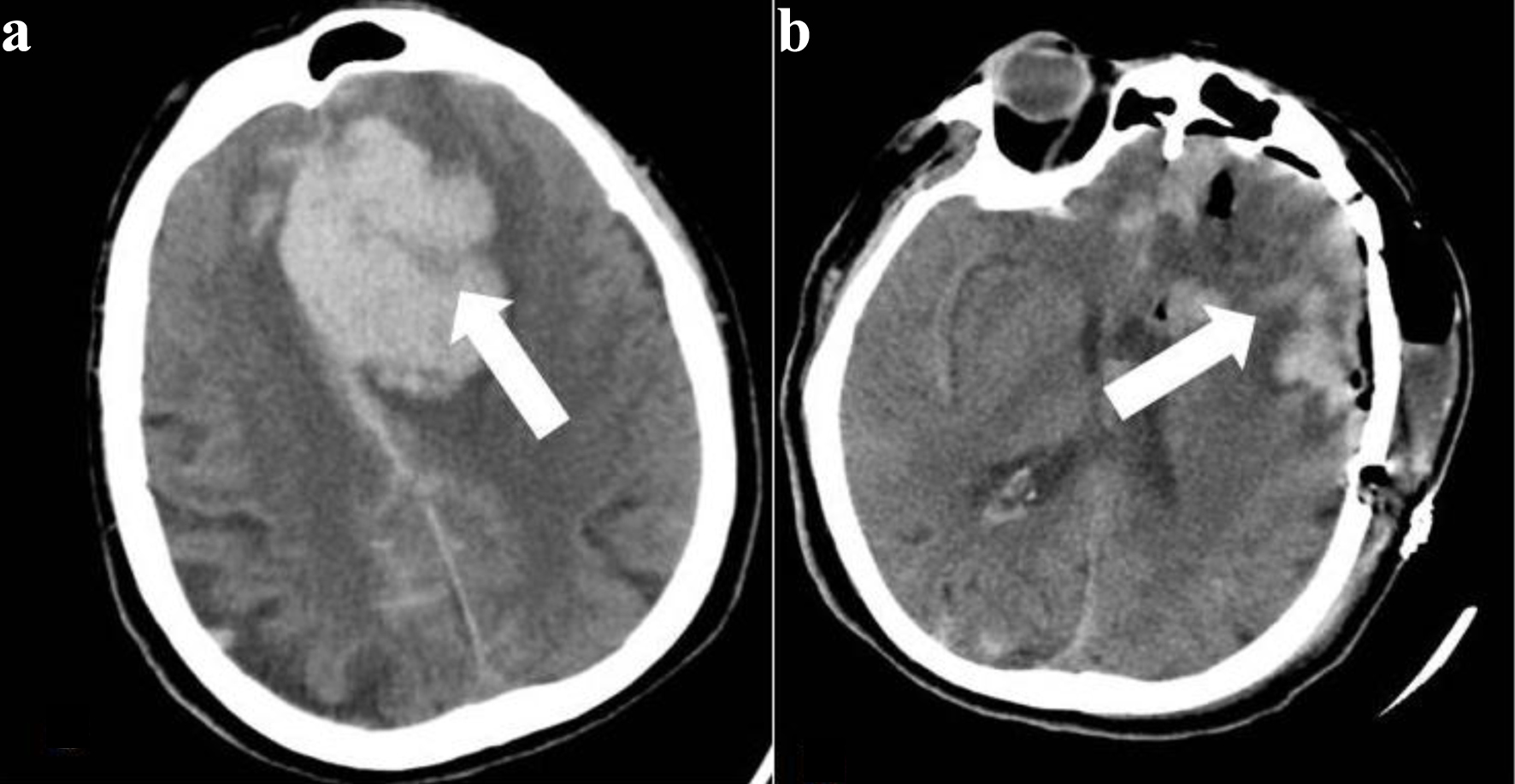 Click for large image | Figure 2. Axial brain computed tomography (CT) sections with a slice thickness of 2.5 mm. (a) The preoperative image demonstrates a hematoma in the left frontal region causing a pronounced midline shift (the white arrow indicates the hemorrhagic area). (b) The 2.5-mm axial brain CT obtained 12 h after surgery shows findings consistent with craniotomy, with a marked regression of the midline shift (the white arrow indicates the surgical site, and the bone flap has been replaced). |
The patients who underwent EVD (n = 21) had a mean age of 67.7 years (range: 33–89; 95% CI: 60.1–75.2; SD: 16.6). Of these patients, 61.9% were female (n = 13) and 38.1% were male (n = 8). While 33.3% of the patients (n = 7) were receiving anticoagulant therapy, 57.1% (n = 12) had a history of antiplatelet or fibrinolytic agent use. Except for one patient, all had various accompanying chronic comorbidities, including hypertension, diabetes mellitus, asthma, thyroid disease, chronic obstructive pulmonary disease, hypercholesterolemia, atrial fibrillation, coronary artery disease, mitral valve prolapse, chronic heart failure, prior ischemic and/or hemorrhagic cerebrovascular disease, history of myelomeningocele surgery, cardiac pacemaker implantation, epilepsy, dementia, benign prostatic hyperplasia, and malignancies such as colon, breast, and lung cancer. The median preoperative GCS score for all patients was 4 (range: 4–9; IQR: 4), while the median early postoperative (first 6 h) GCS score was 6 (range: 4–13; IQR: 5). Ten patients (47.61%) died within the first postoperative month. Within the first 3 months, five of the remaining 11 patients died due to various causes. Among the six surviving patients, four were followed with mild-to-moderate disability, and two with severe disability. Figures 3 illustrates CT images of representative case from our series.
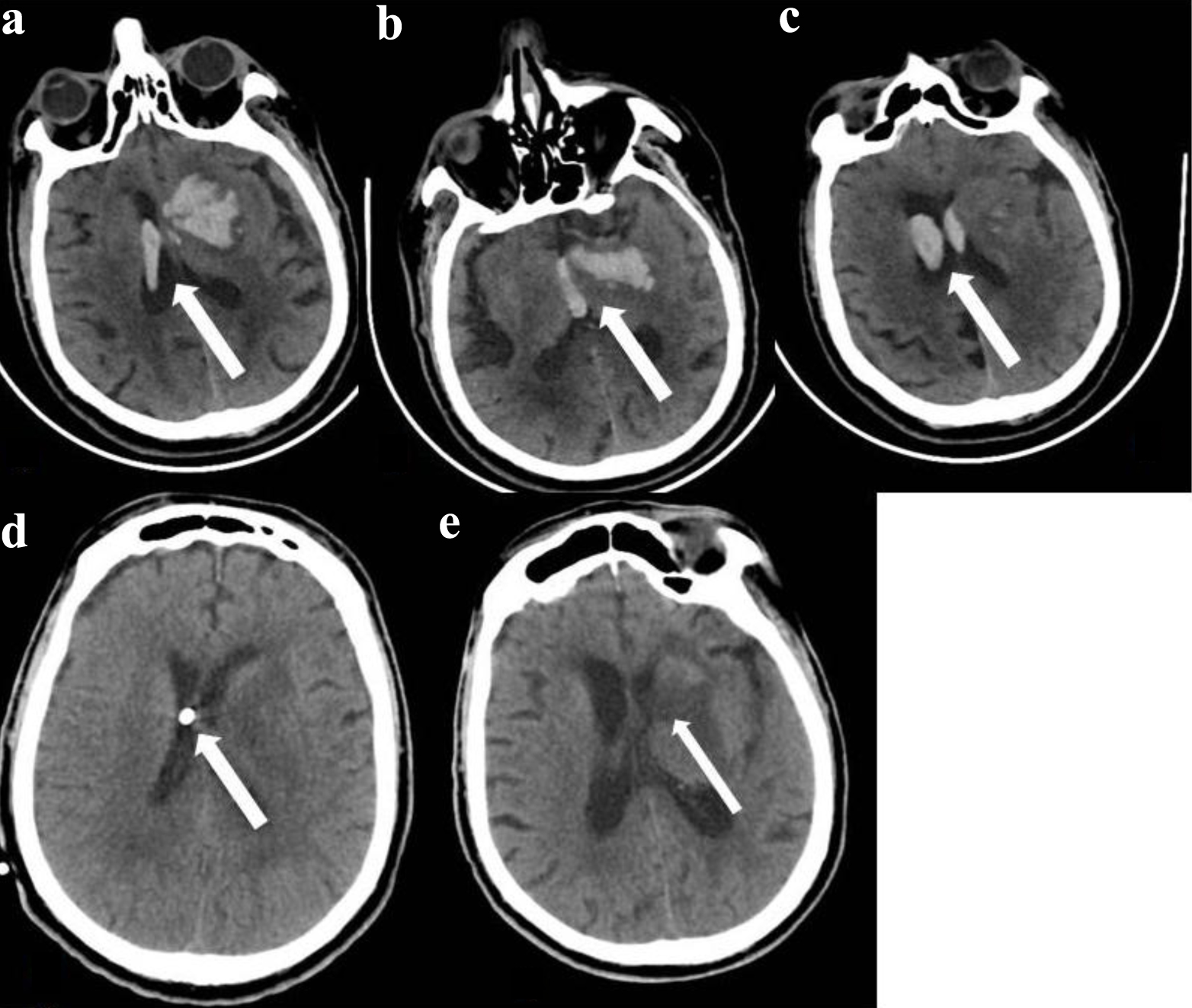 Click for large image | Figure 3. Axial brain computed tomography (CT) sections with a slice thickness of 2.5 mm. (a) Hemorrhage is present in the right lateral ventricle and in the left lateral ventricle with parenchymal involvement (the white arrow indicates the hemorrhage). (b) Hemorrhage is observed in the left lateral ventricle, parenchyma, and the third ventricle (the white arrow indicates the hemorrhage). (c) Hemorrhage is present in both ventricles (the white arrow indicates the hemorrhage). (d) A 2.5-mm axial brain CT image obtained after placement of an external ventricular drainage (EVD) system shows no evidence of intraventricular hemorrhage (the white arrow indicates the ventricular tip of the EVD). (e) Axial brain CT images obtained 25 days after surgery demonstrate complete resorption of the hematoma. The EVD has been removed. An area corresponding to resorption of the parenchymal hematoma is seen in the left frontal region (the white arrow indicates the area of the resorbed parenchymal hematoma). |
Among the five patients who underwent both craniotomy and EVD, three died within the first postoperative month. The remaining two patients were followed with moderate-to-severe disability, with follow-up durations of 10 and 17 months, respectively. Figures 4 illustrates CT images of representative case from our series.
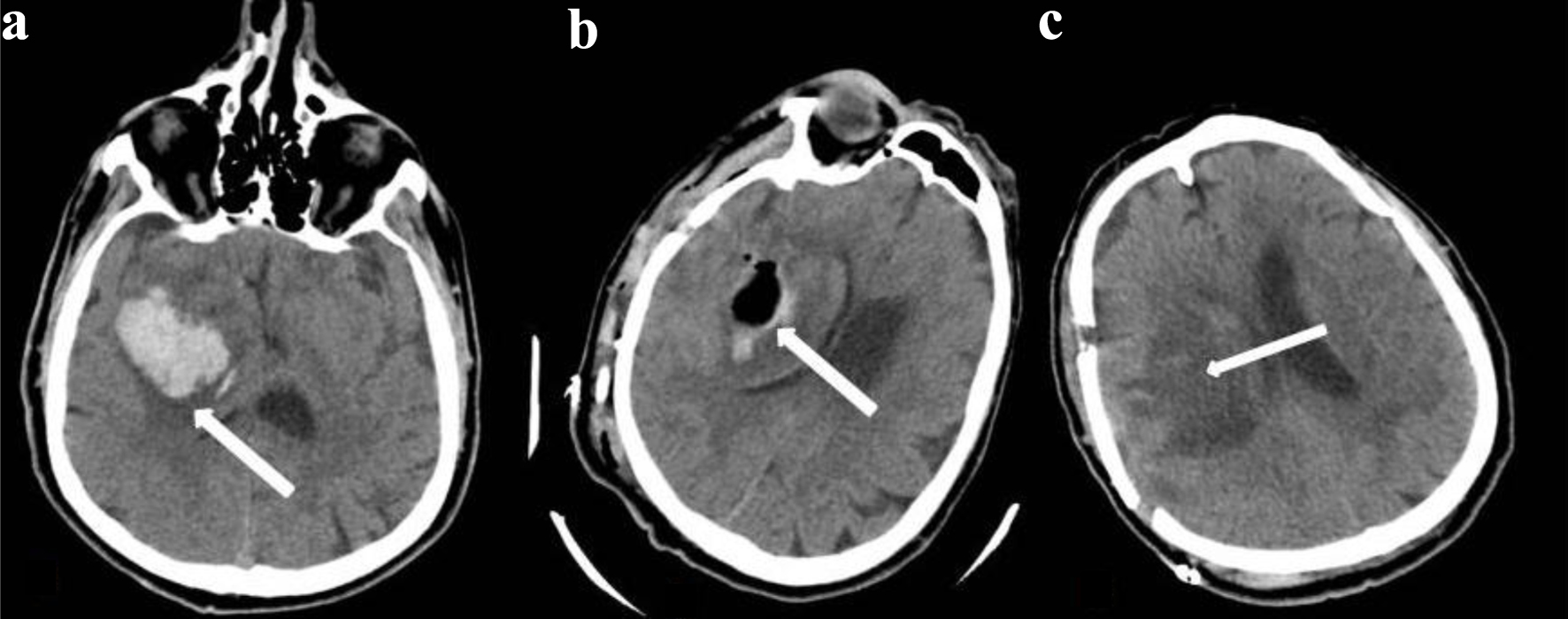 Click for large image | Figure 4. Axial brain computed tomography (CT) sections with a slice thickness of 2.5 mm. (a) A hematoma is present in the right temporal region causing a midline shift (the white arrow indicates the hemorrhage). (b) An axial brain CT obtained 12 h after surgery demonstrates early postoperative changes with regression of the midline shift. The bone flap has been replaced (the white arrow indicates the evacuated hematoma cavity). (c) A 2.5-mm axial brain CT obtained 1 month after surgery shows complete resolution of the hematoma. Bone defects related to the craniotomy are present (the white arrow indicates the previously evacuated hematoma area). |
| Discussion | ▴Top |
The findings of the present study demonstrate that spontaneous ICHs remain associated with substantial morbidity and mortality, with an overall first-month mortality rate of 46.80%. Despite advances in neurosurgical techniques and perioperative intensive care, these outcomes highlight the persistent severity of this clinical entity. Notably, an overwhelming majority of patients (95.74%) had at least one chronic comorbidity, and many had multiple coexisting conditions. This high burden of comorbid disease likely contributes to both the occurrence of hemorrhage and poor clinical outcomes, potentially limiting physiological reserve and recovery capacity. In addition, the widespread use of anticoagulant and antiplatelet/fibrinolytic medications among the study population (82.97%) underscores their significant role as predisposing factors for spontaneous intracerebral hemorrhage. These agents may not only increase the risk of hemorrhage but also exacerbate hematoma expansion and complicate surgical and postoperative management. Taken together, these findings emphasize the importance of careful risk stratification, individualized treatment strategies, and close monitoring of patients with multiple comorbidities and antithrombotic therapy.
Deep perforating vasculopathy, cerebral amyloid angiopathy, arteriovenous malformations, aneurysms, cavernous malformations, intracranial venous thrombosis, dural arteriovenous fistulas, hemorrhagic transformation of cerebral infarction, severe coagulation factor deficiencies such as hemophilia, tumors (primary or metastatic), vasculitis, infective endocarditis, and posterior reversible encephalopathy syndrome may all be considered among the etiologies of ICH [7]. In our study, a wide range of accompanying systemic comorbidities were identified, including not only primary or metastatic brain tumors but also various other malignancies, prior cerebrovascular diseases, and multiple cardiac disorders. Although some of these conditions do not directly involve the brain, it is evident that they may increase the likelihood of hemorrhage by compromising overall physiological resilience or through indirect mechanisms. Additionally, the fact that 82.7% of our patients were receiving anticoagulant and/or antiplatelet/fibrinolytic therapy further supports the notion that antithrombotic treatment substantially contributes to an increased predisposition to intracerebral bleeding.
Prognosis is of critical importance in patients with ICHs, and various scoring systems have been proposed to predict outcomes. Among these, the ICH score is the most widely used prognostic tool, as it integrates demographic and clinical information with the location and volume of the intracerebral hemorrhage, as well as the presence of intraventricular hemorrhage. This scoring system is based on five key criteria: the GCS score, hematoma volume, presence or absence of intraventricular hemorrhage, whether the hematoma is infratentorial, and patient age [13]. Although other scoring systems are also available, it has been reported that none significantly outperform the ICH score in predicting outcomes, particularly early mortality [14]. Although non-contrast CT-based scoring systems, including the CT angiography “spot sign” and other hematoma pattern scores, appear to predict hematoma expansion, they do not surpass established clinical (i.e., neurological severity) and hematoma-related (i.e., hematoma volume and presence of intraventricular hemorrhage) parameters in predicting clinical outcomes [15]. In our study, considering all patients, a high mortality rate of 46.80% was observed within the first month. Similar findings have been reported in the literature. For instance, in a study by Kiyak et al (2024), the overall mortality rate was reported as 62.87% [16]. When examining the potential reasons for this, it should be noted that 21 patients in our second group underwent surgery solely due to intraventricular hemorrhage. The impact of these patients should not be underestimated. The presence of intraventricular hemorrhage has already been reported in the literature as an independent prognostic factor in intracerebral hemorrhage [17]. Additionally, several factors in our cohort likely contributed to poor prognosis. Most patients had very low preoperative GCS scores, and the majority were of advanced age. In particular, among the patients undergoing craniotomy, none had a total hematoma volume below 30 cm3, and all exhibited midline shift, which are recognized predictors of worse outcomes. Furthermore, it is important to emphasize that the type of surgery performed was not the sole determinant of prognosis, including during the first postoperative month. The quality of intensive care and the occurrence of potential infectious complications also play critical roles in influencing patient outcomes.
In certain patient groups with ICHs, evacuation of the hematoma via craniotomy or craniectomy is now considered a conventional and well-established approach [18]. This approach remains important because it can be performed by any neurosurgeon and at any center with intensive care capabilities. Numerous studies in the literature have either supported or questioned the benefit of this surgical intervention. In patients whose condition deteriorates rapidly due to brainstem compression, surgical evacuation of the hematoma is a widely accepted practice, despite the lack of randomized evaluations of this strategy. For supratentorial intracerebral hemorrhage, early evacuation via standard craniotomy (within 24 h of hemorrhage onset) is considered life-saving in patients who are deteriorating; however, its benefit in patients in deep coma or those who are clinically stable is not clearly established [9]. An individual patient data meta-analysis suggests that surgical intervention provides modest overall benefit, with the greatest advantage observed in patients aged 50–69 years who receive early treatment (within 8 h of symptom onset), have medium-sized hematomas (20–50 mL), and present with impaired but responsive consciousness (GCS score 9–12) [19]. In our study, all surgically treated patients had GCS scores of 8 or below, and hematoma volumes ranged from 45 to 150 cm3. Nevertheless, although the literature may appear inconclusive or only modestly encouraging, the primary purpose of surgery in many cases is to give patients a chance for survival. Additionally, medicolegal considerations often influence the decision to operate. Even when patient life expectancy is limited, the potential legal consequences of not performing or recommending surgery may contribute to the decision-making process regarding surgical intervention.
Intraventricular hemorrhage is an independent prognostic factor in intracerebral hemorrhage. This is because blood degradation products can lead to inflammatory meningitis and hydrocephalus, and are associated with worse outcomes when intraventricular blood volume is increased. EVD, with or without controlled irrigation using a lytic agent such as alteplase, can facilitate rapid clearance of intraventricular hemorrhage, thereby improving the chances of survival in patients with deteriorating consciousness [6, 17]. In our study, no irrigation with any lytic agent was performed. EVD was not used as an alternative to craniotomy; it was only applied to patients with isolated intraventricular hemorrhage or hematomas with substantial ventricular extension. Therefore, it is not possible to compare the efficacy of different surgical approaches between our study groups. In this cohort, 47.61% of patients died within the first postoperative month, which is comparable to rates reported in the literature. Additionally, as in other groups, intensive care conditions must be considered among the factors influencing prognosis.
Minimally invasive surgery (MIS), performed by placing a catheter or stylet under non-contrast CT guidance to decompress the hematoma, can be applied in patients with high rates of intracerebral hemorrhage and limited access to neurosurgical care. MIS, employing various techniques, has become a mainstream approach for the surgical treatment of intracerebral hemorrhage—particularly deep-seated hematomas—because it minimizes parenchymal damage during hematoma access. Meta-analyses of clinical studies conducted in diverse settings, comparing stereotactic aspiration or endoscopic drainage with other treatments (including craniotomy and conservative management), have shown that MIS can achieve superior outcomes [10, 20, 21]. In addition, clinical studies are being conducted to evaluate various neurosurgical approaches, including endoscopic hematoma evacuation and MIS using focused ultrasound [7].
Conclusion
In conclusion, ICHs are frequently associated with the use of anticoagulant and antiplatelet/fibrinolytic medications, and these patients often present with multiple comorbidities and various types of cancer. Although mortality and morbidity remain high, particularly in patients presenting with low GCS scores and large hematomas, surgical intervention continues to play a role in providing patients with a chance of survival and in mitigating potential medicolegal consequences.
Acknowledgments
We would like to thank Dr. Fatih Durna and Dr. Ugur Akin for their contribution by allowing the use of data from their patients in our study.
Financial Disclosure
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of Interest
The authors declare no conflict of interest related to this article.
Informed Consent
Not applicable.
Author Contributions
Dr. Hakan Ak: conceptualization, primary manuscript drafting manuscript review, and editing. Dr. Sedanur Ozgul: primary manuscript drafting, data collection, data analysis. Dr. Emine Avgin: data collection, data analysis.
Data Availability
Any inquiries regarding supporting data availability of this study should be directed to the corresponding author.
Artificial Intelligence Usage Statement
ChatGPT (OpenAI) was used to assist with English language translation and editing. The authors reviewed and approved the final version of the manuscript and take full responsibility for its content.
| References | ▴Top |
- Krishnamurthi RV, Feigin VL, Forouzanfar MH, Mensah GA, Connor M, Bennett DA, Moran AE, et al. Global and regional burden of first-ever ischaemic and haemorrhagic stroke during 1990-2010: findings from the Global Burden of Disease Study 2010. Lancet Glob Health. 2013;1(5):e259-281.
doi pubmed - GBD 2019 Stroke Collaborators. Global, regional, and national burden of stroke and its risk factors, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet Neurol. 2021;20(10):795-820.
doi pubmed - Qureshi AI, Mendelow AD, Hanley DF. Intracerebral haemorrhage. Lancet. 2009;373(9675):1632-1644.
doi pubmed - van Asch CJ, Luitse MJ, Rinkel GJ, van der Tweel I, Algra A, Klijn CJ. Incidence, case fatality, and functional outcome of intracerebral haemorrhage over time, according to age, sex, and ethnic origin: a systematic review and meta-analysis. Lancet Neurol. 2010;9(2):167-176.
doi pubmed - Burchell SR, Tang J, Zhang JH. Hematoma expansion following intracerebral hemorrhage: mechanisms targeting the coagulation cascade and platelet activation. Curr Drug Targets. 2017;18(12):1329-1344.
doi pubmed - Hemphill JC, 3rd, Greenberg SM, Anderson CS, Becker K, Bendok BR, Cushman M, Fung GL, et al. Guidelines for the management of spontaneous intracerebral hemorrhage: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2015;46(7):2032-2060.
doi pubmed - Cordonnier C, Demchuk A, Ziai W, Anderson CS. Intracerebral haemorrhage: current approaches to acute management. Lancet. 2018;392(10154):1257-1268.
doi pubmed - Kidwell CS, Chalela JA, Saver JL, Starkman S, Hill MD, Demchuk AM, Butman JA, et al. Comparison of MRI and CT for detection of acute intracerebral hemorrhage. JAMA. 2004;292(15):1823-1830.
doi pubmed - Mendelow AD, Gregson BA, Fernandes HM, Murray GD, Teasdale GM, Hope DT, Karimi A, et al. Early surgery versus initial conservative treatment in patients with spontaneous supratentorial intracerebral haematomas in the International Surgical Trial in Intracerebral Haemorrhage (STICH): a randomised trial. Lancet. 2005;365(9457):387-397.
doi pubmed - Mendelow AD, Gregson BA, Rowan EN, Murray GD, Gholkar A, Mitchell PM, Investigators SI. Early surgery versus initial conservative treatment in patients with spontaneous supratentorial lobar intracerebral haematomas (STICH II): a randomised trial. Lancet. 2013;382(9890):397-408.
doi pubmed - Hanley DF, Thompson RE, Rosenblum M, Yenokyan G, Lane K, McBee N, Mayo SW, et al. Efficacy and safety of minimally invasive surgery with thrombolysis in intracerebral haemorrhage evacuation (MISTIE III): a randomised, controlled, open-label, blinded endpoint phase 3 trial. Lancet. 2019;393(10175):1021-1032.
doi pubmed - Kothari RU, Brott T, Broderick JP, Barsan WG, Sauerbeck LR, Zuccarello M, Khoury J. The ABCs of measuring intracerebral hemorrhage volumes. Stroke. 1996;27(8):1304-1305.
doi pubmed - Hemphill JC, 3rd, Bonovich DC, Besmertis L, Manley GT, Johnston SC. The ICH score: a simple, reliable grading scale for intracerebral hemorrhage. Stroke. 2001;32(4):891-897.
doi pubmed - Heeley E, Anderson CS, Woodward M, Arima H, Robinson T, Stapf C, Parsons M, et al. Poor utility of grading scales in acute intracerebral hemorrhage: results from the INTERACT2 trial. Int J Stroke. 2015;10(7):1101-1107.
doi pubmed - Huynh TJ, Aviv RI, Dowlatshahi D, Gladstone DJ, Laupacis A, Kiss A, Hill MD, et al. Validation of the 9-point and 24-point hematoma expansion prediction scores and derivation of the PREDICT A/B scores. Stroke. 2015;46(11):3105-3110.
doi pubmed - Kiyak V. Spontaneous intracerebral hematoma: a single center 10-year analysis. Dicle Med J. 2024;51(1):28-35.
- Lv XN, Cheng J, Liu XY, Liu JC, Deng L, Li ZQ, Pu MJ, et al. Ultraearly intraventricular hemorrhage growth predicts early neurologic deterioration and poor functional outcome after acute intracerebral hemorrhage. J Am Heart Assoc. 2023;12(21):e031214.
doi pubmed - Bhaskar MK, Kumar R, Ojha B, Singh SK, Verma N, Verma R, Chandra A, et al. A randomized controlled study of operative versus nonoperative treatment for large spontaneous supratentorial intracerebral hemorrhage. Neurol India. 2017;65(4):752-758.
doi pubmed - Gregson BA, Broderick JP, Auer LM, Batjer H, Chen XC, Juvela S, Morgenstern LB, et al. Individual patient data subgroup meta-analysis of surgery for spontaneous supratentorial intracerebral hemorrhage. Stroke. 2012;43(6):1496-1504.
doi pubmed - Li Y, Zhang H, Wang X, She L, Yan Z, Zhang N, Du R, et al. Neuroendoscopic surgery versus external ventricular drainage alone or with intraventricular fibrinolysis for intraventricular hemorrhage secondary to spontaneous supratentorial hemorrhage: a systematic review and meta-analysis. PLoS One. 2013;8(11):e80599.
doi pubmed - Zhou X, Chen J, Li Q, Ren G, Yao G, Liu M, Dong Q, et al. Minimally invasive surgery for spontaneous supratentorial intracerebral hemorrhage: a meta-analysis of randomized controlled trials. Stroke. 2012;43(11):2923-2930.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (CC BY 4.0), which permits unrestricted use, distribution, and reproduction in any medium, including commercial use, provided the original work is properly cited.
Journal of Current Surgery is published by Elmer Press Inc.